Nicole Adams, Nan Kong, Renran Tian, Christelle Altidor, Shen Chang
{"title":"Untrained Bystanders Administering Drone-Delivered Naloxone: An Exploratory Study.","authors":"Nicole Adams, Nan Kong, Renran Tian, Christelle Altidor, Shen Chang","doi":"10.1177/11782218231211830","DOIUrl":null,"url":null,"abstract":"<p><strong>Introduction: </strong>Opioid overdose deaths continue to climb in the United States. Administering naloxone to an overdose victim can save their life, but rapid access to naloxone remains a barrier. Delivering naloxone to a bystander using a drone has potential to increase naloxone availability but there are still many uncertainties about this mode of delivery. Can an untrained bystander to an opioid overdose successfully administer drone delivered naloxone after viewing video instructions on the drone and how long does it take?</p><p><strong>Methods: </strong>This mixed-methods observational study, conducted in a controlled outdoor environment, simulated an opioid overdose using a mannequin (overdose victim) and panicked bystander. Untrained and medically naïve participants were instructed to call for help, move the drone from the landing spot to the mannequin, and follow the instructions provided by the drone to administer naloxone. Data was collected using video recordings, interviews, and an online survey. Time stamp data was extracted from the video for 2 time points: time for removing the naloxone from the drone and time to administer the naloxone. Interviews were audio recorded and analyzed using an inductive concept analysis approach. One interview question was coded as a binary response of anxiety/no anxiety and added to the demographic data.</p><p><strong>Results: </strong>The average time to remove and administer naloxone was 62 seconds. Anxiety during the activity was reported by 59% of the participants but there was no correlation between anxiety and time. The design of our drone and instructional video can be improved.</p><p><strong>Conclusions: </strong>We have established baseline times for completing steps in administering naloxone delivered by drone. We were able to successfully induce anxiety and have a baseline measure for what percentage of untrained bystanders may experience anxiety when involved with an emergency situation. Design of instructional materials and drone construction can contribute to anxiety and successful administration of naloxone.</p>","PeriodicalId":22185,"journal":{"name":"Substance Abuse: Research and Treatment","volume":"17 ","pages":"11782218231211830"},"PeriodicalIF":2.4000,"publicationDate":"2023-11-29","publicationTypes":"Journal Article","fieldsOfStudy":null,"isOpenAccess":false,"openAccessPdf":"https://www.ncbi.nlm.nih.gov/pmc/articles/PMC10687938/pdf/","citationCount":"0","resultStr":null,"platform":"Semanticscholar","paperid":null,"PeriodicalName":"Substance Abuse: Research and Treatment","FirstCategoryId":"1085","ListUrlMain":"https://doi.org/10.1177/11782218231211830","RegionNum":0,"RegionCategory":null,"ArticlePicture":[],"TitleCN":null,"AbstractTextCN":null,"PMCID":null,"EPubDate":"2023/1/1 0:00:00","PubModel":"eCollection","JCR":"Q3","JCRName":"SUBSTANCE ABUSE","Score":null,"Total":0}
引用次数: 0
Abstract
Introduction: Opioid overdose deaths continue to climb in the United States. Administering naloxone to an overdose victim can save their life, but rapid access to naloxone remains a barrier. Delivering naloxone to a bystander using a drone has potential to increase naloxone availability but there are still many uncertainties about this mode of delivery. Can an untrained bystander to an opioid overdose successfully administer drone delivered naloxone after viewing video instructions on the drone and how long does it take?
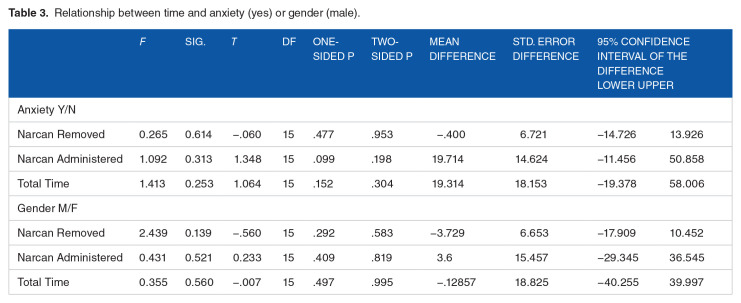
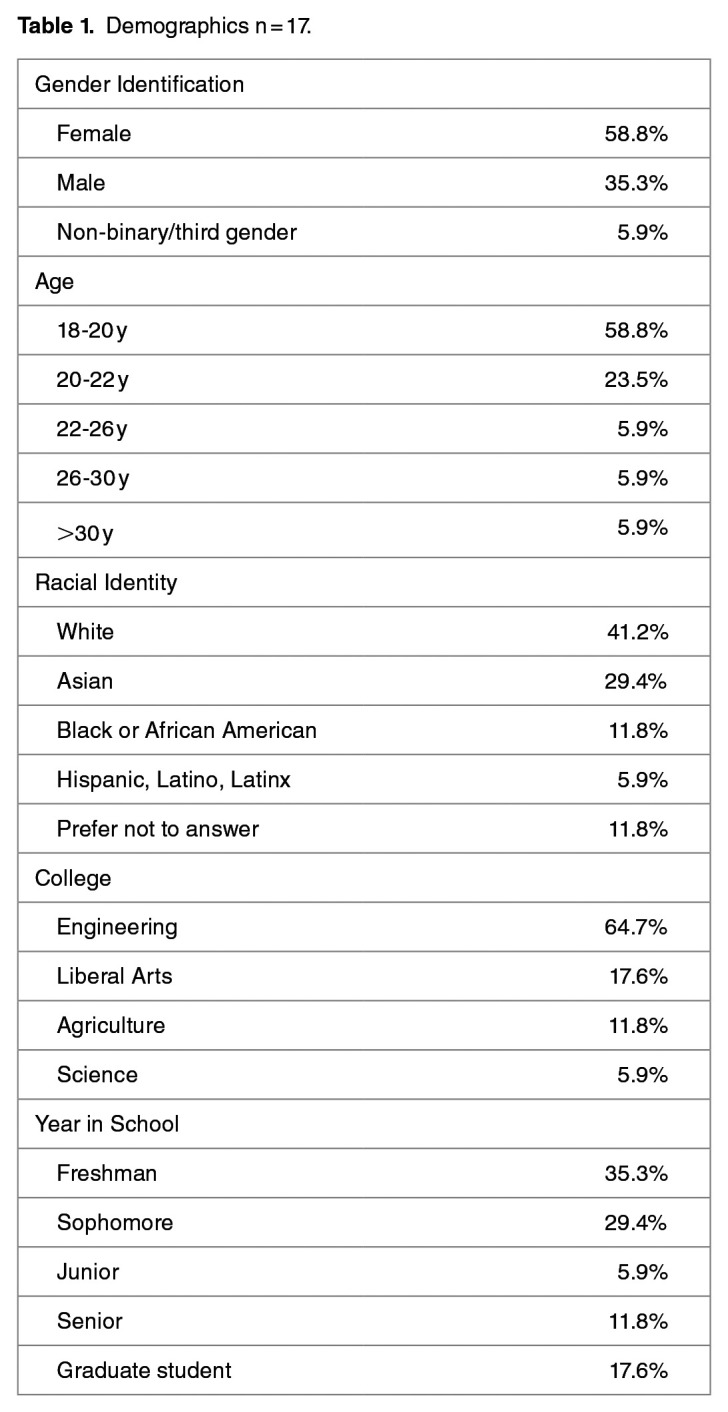
Methods: This mixed-methods observational study, conducted in a controlled outdoor environment, simulated an opioid overdose using a mannequin (overdose victim) and panicked bystander. Untrained and medically naïve participants were instructed to call for help, move the drone from the landing spot to the mannequin, and follow the instructions provided by the drone to administer naloxone. Data was collected using video recordings, interviews, and an online survey. Time stamp data was extracted from the video for 2 time points: time for removing the naloxone from the drone and time to administer the naloxone. Interviews were audio recorded and analyzed using an inductive concept analysis approach. One interview question was coded as a binary response of anxiety/no anxiety and added to the demographic data.
Results: The average time to remove and administer naloxone was 62 seconds. Anxiety during the activity was reported by 59% of the participants but there was no correlation between anxiety and time. The design of our drone and instructional video can be improved.
Conclusions: We have established baseline times for completing steps in administering naloxone delivered by drone. We were able to successfully induce anxiety and have a baseline measure for what percentage of untrained bystanders may experience anxiety when involved with an emergency situation. Design of instructional materials and drone construction can contribute to anxiety and successful administration of naloxone.


 求助内容:
求助内容: 应助结果提醒方式:
应助结果提醒方式:


