Allyson Kis, Tarek Razek, Jeremy Grushka, Nathalie Boulanger, Larry Watt, Dan Deckelbaum, Kosar Khwaja, Paola Fata, Evan G Wong
{"title":"Surgical, trauma and telehealth capacity in Indigenous communities in Northern Quebec: a cross-sectional survey.","authors":"Allyson Kis, Tarek Razek, Jeremy Grushka, Nathalie Boulanger, Larry Watt, Dan Deckelbaum, Kosar Khwaja, Paola Fata, Evan G Wong","doi":"10.1503/cjs.013822","DOIUrl":null,"url":null,"abstract":"<p><strong>Background: </strong>Delivering trauma and surgical care to Northern Quebec presents unique challenges owing to the region's remoteness, extreme weather and limited transport; the expansion of telehealth could help address these difficulties. We aimed to evaluate current surgical, trauma and telemedicine capacity in Nunavik, Quebec.</p><p><strong>Methods: </strong>We used validated assessment tools, including the Personnel, Infrastructure, Procedures, Equipment and Supplies survey, the International Assessment of Capacity for Trauma index and the Maryland Health Care Commission Telemedicine Readiness tool to evaluate surgical, trauma and telemedicine capacity, respectively. We adapted these tools to the Northern Quebec context through discussions with local leadership. Data were collected in 2 regional hospitals - the Ungava Tulattavik Health Centre (UTHC) and the Inuulitsivik Health Centre (IHC) - and 12 Centres locaux de services communautaires (CLSCs; local community services centres) in 6 villages along the Hudson Bay coast and 6 villages along the Ungava Bay coast through iterative discussions with 4 chief nurses from each regional hospital and set of CLSCs; resources were confirmed through on-site evaluation by the respondents. We performed a descriptive analysis of the data.</p><p><strong>Results: </strong>Surgical capacity was highest in the IHC (6.76) and lowest in the Ungava Bay CLSCs (5.52). Personnel (0%-0%) and procedures (13%-33%) were the least available resources. Trauma capacity was highest in the IHC (7.25) and lowest in the Hudson Bay CLSCs (5.58). Although equipment (90%-100%) and supplies (100%-100%) were readily available, personnel (0%-0%) and procedures (25%-56%) were lacking. The UTHC was most prepared for telehealth (67.80%), and the Ungava Bay CLSCs achieved a lower score (51.13%). Underdeveloped telehealth criteria included funding, administrative support, quality improvement and physical spaces (all 33%-67%).</p><p><strong>Conclusion: </strong>Acute care capacity in Nunavik appears heterogeneous, with readily available equipment and supplies, but a lack of personnel capable of performing lifesaving procedures. To address the need for telemedicine, future initiatives should focus on improving funding, administrative support, physical spaces and quality-improvement initiatives.</p>","PeriodicalId":9573,"journal":{"name":"Canadian Journal of Surgery","volume":"66 6","pages":"E572-E579"},"PeriodicalIF":2.2000,"publicationDate":"2023-11-28","publicationTypes":"Journal Article","fieldsOfStudy":null,"isOpenAccess":false,"openAccessPdf":"https://www.ncbi.nlm.nih.gov/pmc/articles/PMC10699286/pdf/","citationCount":"0","resultStr":null,"platform":"Semanticscholar","paperid":null,"PeriodicalName":"Canadian Journal of Surgery","FirstCategoryId":"3","ListUrlMain":"https://doi.org/10.1503/cjs.013822","RegionNum":4,"RegionCategory":"医学","ArticlePicture":[],"TitleCN":null,"AbstractTextCN":null,"PMCID":null,"EPubDate":"2023/11/1 0:00:00","PubModel":"Print","JCR":"Q2","JCRName":"SURGERY","Score":null,"Total":0}
引用次数: 0
Abstract
Background: Delivering trauma and surgical care to Northern Quebec presents unique challenges owing to the region's remoteness, extreme weather and limited transport; the expansion of telehealth could help address these difficulties. We aimed to evaluate current surgical, trauma and telemedicine capacity in Nunavik, Quebec.
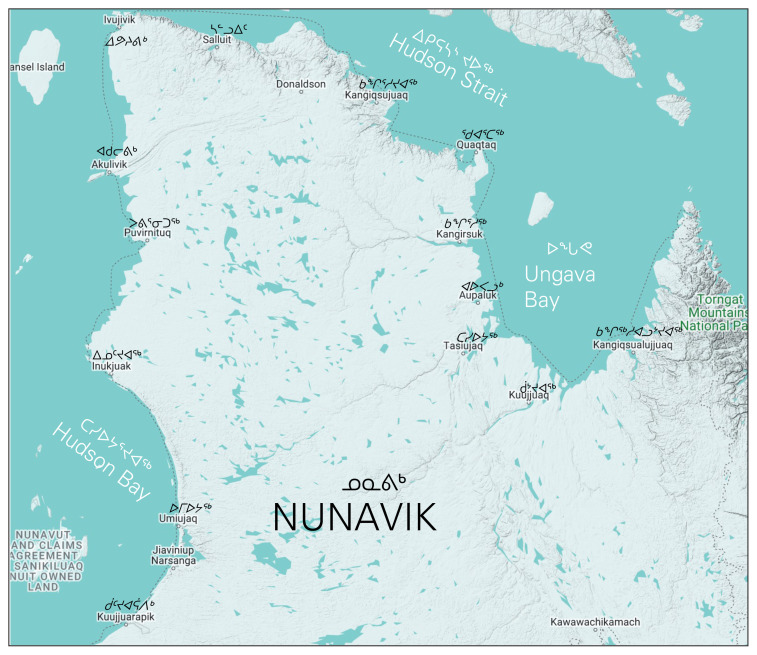
Methods: We used validated assessment tools, including the Personnel, Infrastructure, Procedures, Equipment and Supplies survey, the International Assessment of Capacity for Trauma index and the Maryland Health Care Commission Telemedicine Readiness tool to evaluate surgical, trauma and telemedicine capacity, respectively. We adapted these tools to the Northern Quebec context through discussions with local leadership. Data were collected in 2 regional hospitals - the Ungava Tulattavik Health Centre (UTHC) and the Inuulitsivik Health Centre (IHC) - and 12 Centres locaux de services communautaires (CLSCs; local community services centres) in 6 villages along the Hudson Bay coast and 6 villages along the Ungava Bay coast through iterative discussions with 4 chief nurses from each regional hospital and set of CLSCs; resources were confirmed through on-site evaluation by the respondents. We performed a descriptive analysis of the data.
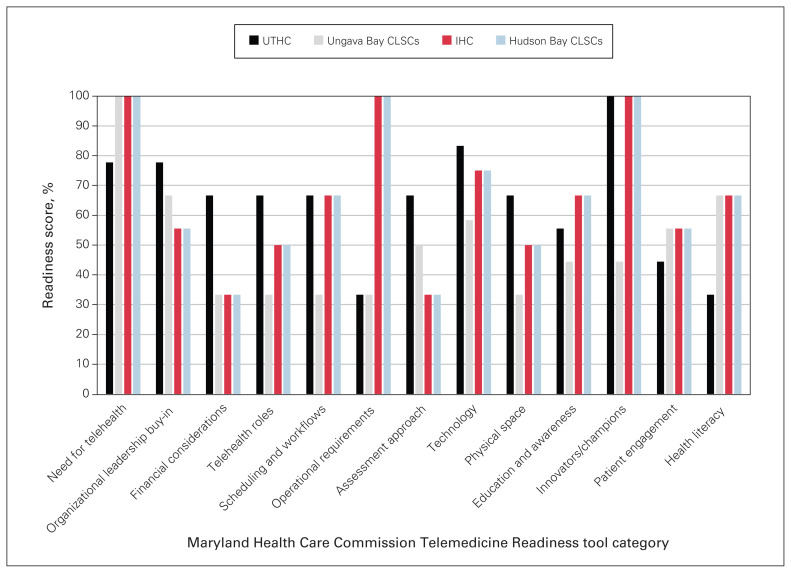
Results: Surgical capacity was highest in the IHC (6.76) and lowest in the Ungava Bay CLSCs (5.52). Personnel (0%-0%) and procedures (13%-33%) were the least available resources. Trauma capacity was highest in the IHC (7.25) and lowest in the Hudson Bay CLSCs (5.58). Although equipment (90%-100%) and supplies (100%-100%) were readily available, personnel (0%-0%) and procedures (25%-56%) were lacking. The UTHC was most prepared for telehealth (67.80%), and the Ungava Bay CLSCs achieved a lower score (51.13%). Underdeveloped telehealth criteria included funding, administrative support, quality improvement and physical spaces (all 33%-67%).
Conclusion: Acute care capacity in Nunavik appears heterogeneous, with readily available equipment and supplies, but a lack of personnel capable of performing lifesaving procedures. To address the need for telemedicine, future initiatives should focus on improving funding, administrative support, physical spaces and quality-improvement initiatives.
背景:由于该地区地处偏远、极端天气和交通有限,向魁北克北部提供创伤和外科护理提出了独特的挑战;扩大远程保健可以帮助解决这些困难。我们旨在评估魁北克省努纳维克目前的外科、创伤和远程医疗能力。方法:我们使用经过验证的评估工具,包括人员、基础设施、程序、设备和用品调查、国际创伤能力评估指数和马里兰州卫生保健委员会远程医疗准备工具,分别评估外科、创伤和远程医疗能力。通过与当地领导的讨论,我们使这些工具适应魁北克北部的情况。数据收集于2家地区医院——Ungava Tulattavik保健中心(UTHC)和Inuulitsivik保健中心(IHC)——和12家社区服务中心(CLSCs);在哈德逊湾沿岸的6个村庄和昂加瓦湾沿岸的6个村庄建立当地社区服务中心),通过与每个地区医院的4名护士长和一套社区服务中心进行反复讨论;资源通过被调查者现场评价确认。我们对资料进行了描述性分析。结果:IHC的手术容量最高(6.76),Ungava Bay CLSCs的手术容量最低(5.52)。人员(0%-0%)和程序(13%-33%)是可用资源最少的。创伤容量在IHC组最高(7.25),在Hudson Bay CLSCs组最低(5.58)。虽然设备(90%-100%)和用品(100%-100%)很容易获得,但人员(0%-0%)和程序(25%-56%)缺乏。UTHC对远程医疗的准备程度最高(67.80%),Ungava Bay CLSCs的准备程度较低(51.13%)。不发达的远程保健标准包括资金、行政支助、质量改进和物理空间(均为33%-67%)。结论:努纳维克的急性护理能力似乎参差不齐,有现成的设备和用品,但缺乏能够执行救生程序的人员。为了满足对远程医疗的需求,未来的举措应侧重于改善供资、行政支助、物理空间和质量改进举措。
期刊介绍:
The mission of CJS is to contribute to the meaningful continuing medical education of Canadian surgical specialists, and to provide surgeons with an effective vehicle for the dissemination of observations in the areas of clinical and basic science research.

 求助内容:
求助内容: 应助结果提醒方式:
应助结果提醒方式:


