Vidya L. Ambati, Tammy H. Cummings, Praveen Yerramothu, Joseph Nguyen, S. Scott Sutton, Brian C. Werner, Joseph Magagnoli
{"title":"Association between haloperidol use and risk of rheumatoid arthritis","authors":"Vidya L. Ambati, Tammy H. Cummings, Praveen Yerramothu, Joseph Nguyen, S. Scott Sutton, Brian C. Werner, Joseph Magagnoli","doi":"10.1002/mef2.66","DOIUrl":null,"url":null,"abstract":"<p>An uncontrolled case-series reported a benefit of haloperidol in rheumatoid arthritis (RA).<span><sup>1</sup></span> A study of the FDA Adverse Events Reporting System reported that among RA patients there were fewer users of antipsychotic drugs, including haloperidol, and concluded that antipsychotic drugs could reduce the risk of developing RA.<span><sup>2</sup></span> However, these results only suggest the converse: that RA is associated with a reduced risk of antipsychotic use; they do not indicate that antipsychotics reduce the risk of RA. The same study also examined a small employee insurance database in Japan and reported an inverse temporal relationship between RA and antipsychotic drugs, including haloperidol. Limitations of these two studies include small size, unverified and incomplete records, lack of correction for sociodemographic or clinical confounders, changing time-trends in prescriptions, and selective loss to follow-up. Therefore, we sought to undertake a robust pharmacoepidemiologic study of whether haloperidol, an FDA-approved drug for the treatment of schizophrenia or Tourette disorder, affects the risk of incident RA in three large nationwide health insurance databases that comprise most of the United States population. We did so with the goal of determining whether an inexpensive drug already in clinical use could be repurposed for RA, a disease that affects tens of millions of people worldwide.</p><p>We studied three health insurance databases: PearlDiver Mariner (2010–2021), IBM Marketscan Research Databases (2006–2020), and Veterans Administration (VA) Health database (2001–2021) (Supporting Information: Tables S1–S4). Inclusion criteria were at least 6 months follow-up, at least 18 years of age, schizophrenia or Tourette disorder diagnosed on two separate occasions, and treatment with antipsychotics. RA before diagnosis of schizophrenia or Tourette disorder was exclusionary (Supporting Information: Figure S1). Disease claims were identified by ICD-9-CM and ICD-10-CM codes. Drug exposure was determined by prescriptions for generic or brand versions. Time from first prescription of antipsychotics to diagnosis of RA was the dependent variable. Sensitivity analyses were performed using diagnosis of schizophrenia or Tourette disorder as the index date and flagging treatment with antipsychotics within 60 days of schizophrenia or Tourette disorder diagnosis. Patients were censored when they developed RA, unenrolled, died, or switched between study medication groups. Cox proportional hazards regression analyses were performed to estimate the hazard of RA in relation to haloperidol use. We performed propensity score matching to create cohorts with similar baseline characteristics, reducing possible bias in estimating treatment effects. Additionally, to control for any residual covariate imbalance, we adjusted for RA-associated confounders: age, sex, smoking, body mass index, Charlson comorbidity index, and database entry year. Fine-Gray subdistribution hazard ratios for competing risk of mortality, corrected for covariates, were calculated for the VA, which contains mortality data. We performed inverse-variance weighted meta-analyses to estimate the combined hazard ratio (HR) and 95% confidence intervals (CI) using a random-effects model, computed prediction intervals, and Kaplan–Meier survival analyses.</p><p>The adjusted Cox proportional hazards regression models in the propensity-score-matched populations showed a protective association of haloperidol use against incident RA in each of the three databases (Figure 1A,B). The meta-analyses identified a protective effect of haloperidol in the main (pooled adjusted hazard ratio [aHR] = 0.69; 95% CI: 0.61–0.79; <i>p</i> = 0.0001) and sensitivity analyses (pooled aHR = 0.69; 95% CI: 0.58–0.81; <i>p</i> < 0.0001) (Figure 1A,B). The 95% prediction intervals for the hazard ratio, which provide insights into the range of outcomes in a hypothetical future study, were <1.0 in both analyses (Figure 1A,B), implying a future clinical trial would be estimated to have a >95% probability of identifying a protective effect. Subdistribution hazard ratios, accounting for the competing risk of mortality, in the VA revealed a protective effect (main analysis: aHR = 0.52; 95% CI: 0.27–0.98; <i>p</i> = 0.0002; sensitivity analysis: aHR = 0.48; 95% CI: 0.30–0.76; <i>p</i> = 0.0002). Kaplan–Meier survival analyses revealed that haloperidol use was associated with a lower risk of incident RA in all three databases in both analyses (Figure 1C,D).</p><p>We identified a significant association between haloperidol use and incident RA. Strengths of our study include replication in three cohorts that comprise most United States adults, adjustment for confounders, and propensity score matching, which simulates randomization and increases its validity. As this retrospective study was not randomized, there could be residual confounding or selection bias.</p><p>Haloperidol is reported to inhibit the cytokines interleukin-1β (IL-1β), IL-6, and tumor necrosis factor-α,<span><sup>3, 4</sup></span> which are known drivers of RA.<span><sup>5</sup></span> Dendritic cells and T helper 1 lymphocytes play crucial roles in the pathogenesis of RA.<span><sup>6</sup></span> Haloperidol suppresses the maturation and priming of these cells, respectively.<span><sup>7</sup></span> Together, such effects could, in part, underlie the mechanistic basis of how haloperidol exposure reduces the development of RA. Clinical studies in individuals with mental illness may face ethical challenges as well as recruitment challenges owing to the incidence in this population. However, taken together with the anti-inflammatory effects of haloperidol, our findings, which suggest a potential benefit of haloperidol in RA, provide a rationale for randomized controlled trials in a general population at risk for RA. Such prospective trials could provide causal insights.</p><p><b>Vidya L. Ambati</b>: Conceptualization (equal); data curation (equal); formal analysis (equal); funding acquisition (equal); methodology (equal); writing—original draft (equal); writing—review & editing (equal). <b>Tammy H. Cummings</b>: Methodology (equal); writing—review and editing (equal). <b>Praveen Yerramothu</b>: Data curation (equal); writing—review and editing (equal). <b>Joseph Nguyen</b>: Data curation (equal); writing—review and editing. <b>S. Scott Sutton</b>: Data curation (equal); funding acquisition; methodology (equal); writing—original draft (equal); writing—review and editing. <b>Brian C. Werner</b>: Conceptualization (equal); data curation (equal); funding acquisition; methodology (equal); supervision (equal); writing—original draft (equal); writing—review and editing. <b>Joseph Magagnoli</b>: Conceptualization (equal); data curation (equal); formal analysis (equal); funding acquisition; methodology (equal); supervision (equal); writing—original draft (equal); writing—review and editing (equal). All authors have read and approved the final manuscript.</p><p>S. Scott Sutton has received research grants from Boehringer Ingelheim, Coherus BioSciences, EMD Serono, and Alexion Pharmaceuticals, all for projects unrelated to study. Brian C. Werner and Vidya L. Ambati are named as inventors on matter-related patent applications filed by their university.</p><p>PearlDiver Mariner and IBM Marketscan Research Databases contained deidentified data deemed exempt by the University of Virginia Institutional Review Board (IRB). Veterans Administration (VA) Health database data analysis was compliant with Department of Veterans Affairs requirements and received IRB (1139248-1) and Research and Development Approval.</p>","PeriodicalId":74135,"journal":{"name":"MedComm - Future medicine","volume":"2 4","pages":""},"PeriodicalIF":0.0000,"publicationDate":"2023-11-24","publicationTypes":"Journal Article","fieldsOfStudy":null,"isOpenAccess":false,"openAccessPdf":"https://onlinelibrary.wiley.com/doi/epdf/10.1002/mef2.66","citationCount":"0","resultStr":null,"platform":"Semanticscholar","paperid":null,"PeriodicalName":"MedComm - Future medicine","FirstCategoryId":"1085","ListUrlMain":"https://onlinelibrary.wiley.com/doi/10.1002/mef2.66","RegionNum":0,"RegionCategory":null,"ArticlePicture":[],"TitleCN":null,"AbstractTextCN":null,"PMCID":null,"EPubDate":"","PubModel":"","JCR":"","JCRName":"","Score":null,"Total":0}
引用次数: 0
Abstract
An uncontrolled case-series reported a benefit of haloperidol in rheumatoid arthritis (RA).1 A study of the FDA Adverse Events Reporting System reported that among RA patients there were fewer users of antipsychotic drugs, including haloperidol, and concluded that antipsychotic drugs could reduce the risk of developing RA.2 However, these results only suggest the converse: that RA is associated with a reduced risk of antipsychotic use; they do not indicate that antipsychotics reduce the risk of RA. The same study also examined a small employee insurance database in Japan and reported an inverse temporal relationship between RA and antipsychotic drugs, including haloperidol. Limitations of these two studies include small size, unverified and incomplete records, lack of correction for sociodemographic or clinical confounders, changing time-trends in prescriptions, and selective loss to follow-up. Therefore, we sought to undertake a robust pharmacoepidemiologic study of whether haloperidol, an FDA-approved drug for the treatment of schizophrenia or Tourette disorder, affects the risk of incident RA in three large nationwide health insurance databases that comprise most of the United States population. We did so with the goal of determining whether an inexpensive drug already in clinical use could be repurposed for RA, a disease that affects tens of millions of people worldwide.
We studied three health insurance databases: PearlDiver Mariner (2010–2021), IBM Marketscan Research Databases (2006–2020), and Veterans Administration (VA) Health database (2001–2021) (Supporting Information: Tables S1–S4). Inclusion criteria were at least 6 months follow-up, at least 18 years of age, schizophrenia or Tourette disorder diagnosed on two separate occasions, and treatment with antipsychotics. RA before diagnosis of schizophrenia or Tourette disorder was exclusionary (Supporting Information: Figure S1). Disease claims were identified by ICD-9-CM and ICD-10-CM codes. Drug exposure was determined by prescriptions for generic or brand versions. Time from first prescription of antipsychotics to diagnosis of RA was the dependent variable. Sensitivity analyses were performed using diagnosis of schizophrenia or Tourette disorder as the index date and flagging treatment with antipsychotics within 60 days of schizophrenia or Tourette disorder diagnosis. Patients were censored when they developed RA, unenrolled, died, or switched between study medication groups. Cox proportional hazards regression analyses were performed to estimate the hazard of RA in relation to haloperidol use. We performed propensity score matching to create cohorts with similar baseline characteristics, reducing possible bias in estimating treatment effects. Additionally, to control for any residual covariate imbalance, we adjusted for RA-associated confounders: age, sex, smoking, body mass index, Charlson comorbidity index, and database entry year. Fine-Gray subdistribution hazard ratios for competing risk of mortality, corrected for covariates, were calculated for the VA, which contains mortality data. We performed inverse-variance weighted meta-analyses to estimate the combined hazard ratio (HR) and 95% confidence intervals (CI) using a random-effects model, computed prediction intervals, and Kaplan–Meier survival analyses.
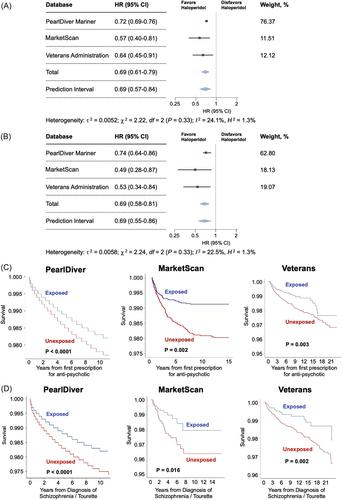
The adjusted Cox proportional hazards regression models in the propensity-score-matched populations showed a protective association of haloperidol use against incident RA in each of the three databases (Figure 1A,B). The meta-analyses identified a protective effect of haloperidol in the main (pooled adjusted hazard ratio [aHR] = 0.69; 95% CI: 0.61–0.79; p = 0.0001) and sensitivity analyses (pooled aHR = 0.69; 95% CI: 0.58–0.81; p < 0.0001) (Figure 1A,B). The 95% prediction intervals for the hazard ratio, which provide insights into the range of outcomes in a hypothetical future study, were <1.0 in both analyses (Figure 1A,B), implying a future clinical trial would be estimated to have a >95% probability of identifying a protective effect. Subdistribution hazard ratios, accounting for the competing risk of mortality, in the VA revealed a protective effect (main analysis: aHR = 0.52; 95% CI: 0.27–0.98; p = 0.0002; sensitivity analysis: aHR = 0.48; 95% CI: 0.30–0.76; p = 0.0002). Kaplan–Meier survival analyses revealed that haloperidol use was associated with a lower risk of incident RA in all three databases in both analyses (Figure 1C,D).
We identified a significant association between haloperidol use and incident RA. Strengths of our study include replication in three cohorts that comprise most United States adults, adjustment for confounders, and propensity score matching, which simulates randomization and increases its validity. As this retrospective study was not randomized, there could be residual confounding or selection bias.
Haloperidol is reported to inhibit the cytokines interleukin-1β (IL-1β), IL-6, and tumor necrosis factor-α,3, 4 which are known drivers of RA.5 Dendritic cells and T helper 1 lymphocytes play crucial roles in the pathogenesis of RA.6 Haloperidol suppresses the maturation and priming of these cells, respectively.7 Together, such effects could, in part, underlie the mechanistic basis of how haloperidol exposure reduces the development of RA. Clinical studies in individuals with mental illness may face ethical challenges as well as recruitment challenges owing to the incidence in this population. However, taken together with the anti-inflammatory effects of haloperidol, our findings, which suggest a potential benefit of haloperidol in RA, provide a rationale for randomized controlled trials in a general population at risk for RA. Such prospective trials could provide causal insights.
Vidya L. Ambati: Conceptualization (equal); data curation (equal); formal analysis (equal); funding acquisition (equal); methodology (equal); writing—original draft (equal); writing—review & editing (equal). Tammy H. Cummings: Methodology (equal); writing—review and editing (equal). Praveen Yerramothu: Data curation (equal); writing—review and editing (equal). Joseph Nguyen: Data curation (equal); writing—review and editing. S. Scott Sutton: Data curation (equal); funding acquisition; methodology (equal); writing—original draft (equal); writing—review and editing. Brian C. Werner: Conceptualization (equal); data curation (equal); funding acquisition; methodology (equal); supervision (equal); writing—original draft (equal); writing—review and editing. Joseph Magagnoli: Conceptualization (equal); data curation (equal); formal analysis (equal); funding acquisition; methodology (equal); supervision (equal); writing—original draft (equal); writing—review and editing (equal). All authors have read and approved the final manuscript.
S. Scott Sutton has received research grants from Boehringer Ingelheim, Coherus BioSciences, EMD Serono, and Alexion Pharmaceuticals, all for projects unrelated to study. Brian C. Werner and Vidya L. Ambati are named as inventors on matter-related patent applications filed by their university.
PearlDiver Mariner and IBM Marketscan Research Databases contained deidentified data deemed exempt by the University of Virginia Institutional Review Board (IRB). Veterans Administration (VA) Health database data analysis was compliant with Department of Veterans Affairs requirements and received IRB (1139248-1) and Research and Development Approval.

 求助内容:
求助内容: 应助结果提醒方式:
应助结果提醒方式:


