Fighting to Breathe and Fighting for Health-Related Quality of Life: Measuring the Impact of Being Dependent on Technology for Breathing on the Child and Their Caregiver.
Janine Verstraete, Christopher Booth, Jane Booth, Shazia Peer, Jessica McGuire, Fiona Kritzinger, Taryn Gray, Noluthando Zibi, Primrose Shabangu, Marco Zampoli
{"title":"Fighting to Breathe and Fighting for Health-Related Quality of Life: Measuring the Impact of Being Dependent on Technology for Breathing on the Child and Their Caregiver.","authors":"Janine Verstraete, Christopher Booth, Jane Booth, Shazia Peer, Jessica McGuire, Fiona Kritzinger, Taryn Gray, Noluthando Zibi, Primrose Shabangu, Marco Zampoli","doi":"10.1007/s40271-023-00657-4","DOIUrl":null,"url":null,"abstract":"<p><strong>Background and objective: </strong>Medical advancement has enabled children to survive congenital airway anomalies, rare diseases and critical illnesses with medical technology including tracheostomies and long-term ventilation to support breathing. This study aimed to assess (1) the validity of the EQ-TIPS and EQ-5D-Y-3L in children dependent on technology and (2) the impact of caring for these children on the EQ-5D-5L and CarerQoL.</p><p><strong>Methods: </strong>Caregivers of children aged 1 month to 18 years completed the EQ-TIPS or EQ-5D-Y-3L, Pediatric Quality of Life Inventory (PedsQL) and Paediatric Tracheostomy Health Status Instrument (PTHSI) to reflect the child's health. In addition, caregivers self-completed the EQ-5D-5L and CarerQoL. Reports of problems on EQ dimensions were compared across age groups with the Fisher's exact test. Spearman and Pearson's correlation coefficients and Kruskal-Wallis H-test were used to explore the association between caregiver and child scores, concurrent validity, and known-group validity of the EQ-TIPS and EQ-5D-Y-3L.</p><p><strong>Results: </strong>Responses from 144 caregivers were collected, 66 for children aged 1 month to 4 years completing EQ-TIPS and 78 for children aged 5-18 years completing EQ-5D-Y-3L. The EQ-TIPS showed a higher report of no problems for social interaction for children aged 1-12 months (p = 0.040) than the older age groups, there were however no differences in the level sum score (LSS) or EQ Visual Analogue Scale scores between the age groups. The EQ-5D-Y-3L showed a significantly less report of problems for mobility (p = 0.013) and usual activities (p = 0.006) for children aged 5-7 years compared with children aged 8-12 and children aged 13-18 years. Similarly, the 5-7 years of age group had a significantly lower EQ-5D-Y-3L LSS compared with the older groups (H = 12.08, p = 0.002). The EQ-TIPS and EQ-5D-Y-3L showed moderate-to-strong associations with the PedsQL. EQ-TIPS median LSS was able to differentiate between groups on the clinical prognosis with a better health-related quality of life (HRQoL) in those where weaning from technology is possible compared with those where weaning is not possible (H = 18.98, p = 0.011). The EQ-5D-Y-3L can discriminate between breathing technology, where those with only a tracheostomy reported better HRQoL (H = 8.92, p = 0.012), and between mild and moderate clinical severity (H = 19.42, p < 0.001). Neither the PedsQL nor the PTHSI was able to discriminate between these groups across the age range. Caregiver and child HRQoL scores showed moderate-to-strong associations.</p><p><strong>Conclusions: </strong>The EQ-TIPS and EQ-5D-Y-3L showed good validity in children dependent on the technology for breathing. The EQ-TIPS and EQ-5D-Y-3L LSS were all able to differentiate between children with known clinical variables and outperformed both the PedsQL and PTHSI, making them preferable for intervention research. The caregiver scores are associated with the child HRQoL scores and thus a spill-over should be accounted for in any interventions targeting this cohort. It is recommended that future studies investigate the reliability and responsiveness of these measures in children dependent on technology for breathing.</p>","PeriodicalId":51271,"journal":{"name":"Patient-Patient Centered Outcomes Research","volume":" ","pages":"65-82"},"PeriodicalIF":3.1000,"publicationDate":"2024-01-01","publicationTypes":"Journal Article","fieldsOfStudy":null,"isOpenAccess":false,"openAccessPdf":"https://www.ncbi.nlm.nih.gov/pmc/articles/PMC10769921/pdf/","citationCount":"0","resultStr":null,"platform":"Semanticscholar","paperid":null,"PeriodicalName":"Patient-Patient Centered Outcomes Research","FirstCategoryId":"3","ListUrlMain":"https://doi.org/10.1007/s40271-023-00657-4","RegionNum":3,"RegionCategory":"医学","ArticlePicture":[],"TitleCN":null,"AbstractTextCN":null,"PMCID":null,"EPubDate":"2023/11/22 0:00:00","PubModel":"Epub","JCR":"Q1","JCRName":"HEALTH CARE SCIENCES & SERVICES","Score":null,"Total":0}
引用次数: 0
Abstract
Background and objective: Medical advancement has enabled children to survive congenital airway anomalies, rare diseases and critical illnesses with medical technology including tracheostomies and long-term ventilation to support breathing. This study aimed to assess (1) the validity of the EQ-TIPS and EQ-5D-Y-3L in children dependent on technology and (2) the impact of caring for these children on the EQ-5D-5L and CarerQoL.
Methods: Caregivers of children aged 1 month to 18 years completed the EQ-TIPS or EQ-5D-Y-3L, Pediatric Quality of Life Inventory (PedsQL) and Paediatric Tracheostomy Health Status Instrument (PTHSI) to reflect the child's health. In addition, caregivers self-completed the EQ-5D-5L and CarerQoL. Reports of problems on EQ dimensions were compared across age groups with the Fisher's exact test. Spearman and Pearson's correlation coefficients and Kruskal-Wallis H-test were used to explore the association between caregiver and child scores, concurrent validity, and known-group validity of the EQ-TIPS and EQ-5D-Y-3L.
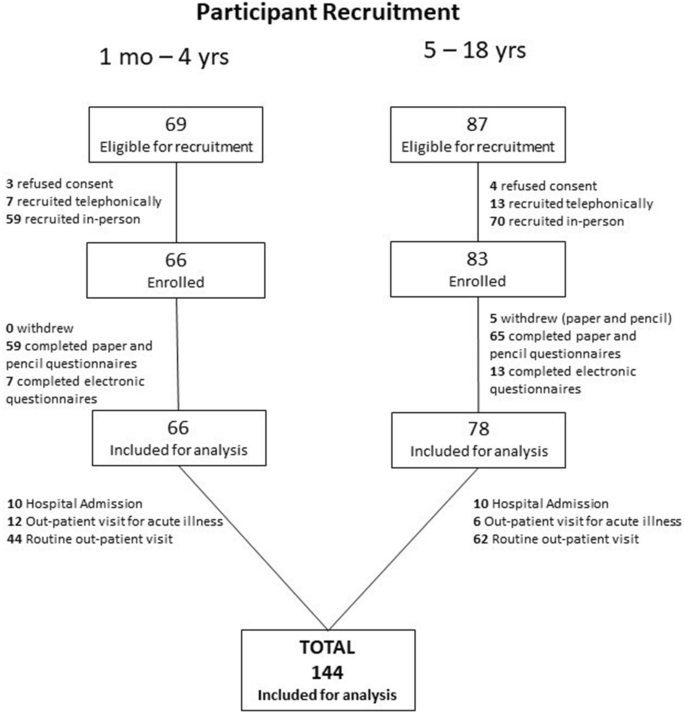
Results: Responses from 144 caregivers were collected, 66 for children aged 1 month to 4 years completing EQ-TIPS and 78 for children aged 5-18 years completing EQ-5D-Y-3L. The EQ-TIPS showed a higher report of no problems for social interaction for children aged 1-12 months (p = 0.040) than the older age groups, there were however no differences in the level sum score (LSS) or EQ Visual Analogue Scale scores between the age groups. The EQ-5D-Y-3L showed a significantly less report of problems for mobility (p = 0.013) and usual activities (p = 0.006) for children aged 5-7 years compared with children aged 8-12 and children aged 13-18 years. Similarly, the 5-7 years of age group had a significantly lower EQ-5D-Y-3L LSS compared with the older groups (H = 12.08, p = 0.002). The EQ-TIPS and EQ-5D-Y-3L showed moderate-to-strong associations with the PedsQL. EQ-TIPS median LSS was able to differentiate between groups on the clinical prognosis with a better health-related quality of life (HRQoL) in those where weaning from technology is possible compared with those where weaning is not possible (H = 18.98, p = 0.011). The EQ-5D-Y-3L can discriminate between breathing technology, where those with only a tracheostomy reported better HRQoL (H = 8.92, p = 0.012), and between mild and moderate clinical severity (H = 19.42, p < 0.001). Neither the PedsQL nor the PTHSI was able to discriminate between these groups across the age range. Caregiver and child HRQoL scores showed moderate-to-strong associations.
Conclusions: The EQ-TIPS and EQ-5D-Y-3L showed good validity in children dependent on the technology for breathing. The EQ-TIPS and EQ-5D-Y-3L LSS were all able to differentiate between children with known clinical variables and outperformed both the PedsQL and PTHSI, making them preferable for intervention research. The caregiver scores are associated with the child HRQoL scores and thus a spill-over should be accounted for in any interventions targeting this cohort. It is recommended that future studies investigate the reliability and responsiveness of these measures in children dependent on technology for breathing.
期刊介绍:
The Patient provides a venue for scientifically rigorous, timely, and relevant research to promote the development, evaluation and implementation of therapies, technologies, and innovations that will enhance the patient experience. It is an international forum for research that advances and/or applies qualitative or quantitative methods to promote the generation, synthesis, or interpretation of evidence.
The journal has specific interest in receiving original research, reviews and commentaries related to qualitative and mixed methods research, stated-preference methods, patient reported outcomes, and shared decision making.
Advances in regulatory science, patient-focused drug development, patient-centered benefit-risk and health technology assessment will also be considered.
Additional digital features (including animated abstracts, video abstracts, slide decks, audio slides, instructional videos, infographics, podcasts and animations) can be published with articles; these are designed to increase the visibility, readership and educational value of the journal’s content. In addition, articles published in The Patient may be accompanied by plain language summaries to assist readers who have some knowledge of, but not in-depth expertise in, the area to understand important medical advances.
All manuscripts are subject to peer review by international experts.

 求助内容:
求助内容: 应助结果提醒方式:
应助结果提醒方式:


