{"title":"Isolated superior mesenteric artery dissection as a cause of abdominal pain","authors":"Leslie Zhi Wei Lew, Zi Qin Ng, Sze Ling Wong","doi":"10.1002/aid2.13377","DOIUrl":null,"url":null,"abstract":"<p>A 50-year-old male presented with sudden onset of upper abdominal pain. He had no infectious or other gastrointestinal symptoms. He had a background of hypertension, hypercholesterolemia and was a heavy smoker. Biochemistry results showed raised white cell count of 28 × 10<sup>9</sup>/L, elevated creatinine of 130 μmol/L, and venous lactate of 4.7 mmol/L.</p><p>Computed tomography (CT) of the abdomen demonstrated a hematoma contained within the lesser sac (Figure 1A). Computed tomography angiography (CTA) revealed an abrupt cutoff of the first branch of superior mesenteric artery (SMA) at the site of hemorrhage suggesting dissection with a distal nonocclusive thrombus (Figures 1B and 2). It was possible that the SMA dissection led to the hematoma within the lesser sac and had tamponade itself. Therefore, there was no active hemorrhage on the subsequent CTA. Given that he was hemodynamically stable with no signs of peritonism, he was managed nonoperatively. He was commenced on lifelong antiplatelet therapy. He had a follow-up CTA which was unremarkable. He remained clinically well.</p><p>Patients with isolated superior mesenteric artery dissection (ISMAD) are at risk of intestinal ischemia. Patients usually present with intractable abdominal pain. Other symptoms include diarrhea, nausea, and vomiting. Risk factors for ISMAD include atherosclerotic disease, hypertension, and abdominal aortic aneurysm.<span><sup>1</sup></span> CTA is the gold standard for diagnosis. Other imaging modalities include ultrasound and magnetic resonance angiography.<span><sup>2</sup></span></p><p>The management of ISMAD consists of initial resuscitation. Patients with no signs of hemodynamic instability or peritonism can be managed nonoperatively.<span><sup>3</sup></span> Anticoagulation is the mainstay of nonoperative management. A systematic review and meta-analysis reported that the majority of patients were commenced on anticoagulation therapy.<span><sup>4</sup></span> Antiplatelet therapy has also been used in stable ISMAD patients with success.<span><sup>5</sup></span></p><p>Operative management options include surgical or endovascular revascularization. Bypass grafting is the most common surgical procedure. Other surgical methods include thrombectomy or ligation of a branch of SMA.<span><sup>4</sup></span></p><p>In conclusion, ISMAD is a rare cause of abdominal pain and prompt treatment is vital due to the risk of intestinal ischemia.</p><p>The authors declare no conflicts of interest.</p><p>According to the Institutional Review Board (IRB), there is no need for IRB approval for an image review article. A written informed consent was obtained from the patient before starting and the authors followed the principles outlined in the WMA Declaration of Helsinki throughout the writing process.</p>","PeriodicalId":7278,"journal":{"name":"Advances in Digestive Medicine","volume":"11 1","pages":"55-56"},"PeriodicalIF":0.4000,"publicationDate":"2023-10-05","publicationTypes":"Journal Article","fieldsOfStudy":null,"isOpenAccess":false,"openAccessPdf":"https://onlinelibrary.wiley.com/doi/epdf/10.1002/aid2.13377","citationCount":"0","resultStr":null,"platform":"Semanticscholar","paperid":null,"PeriodicalName":"Advances in Digestive Medicine","FirstCategoryId":"1085","ListUrlMain":"https://onlinelibrary.wiley.com/doi/10.1002/aid2.13377","RegionNum":0,"RegionCategory":null,"ArticlePicture":[],"TitleCN":null,"AbstractTextCN":null,"PMCID":null,"EPubDate":"","PubModel":"","JCR":"Q4","JCRName":"GASTROENTEROLOGY & HEPATOLOGY","Score":null,"Total":0}
引用次数: 0
Abstract
A 50-year-old male presented with sudden onset of upper abdominal pain. He had no infectious or other gastrointestinal symptoms. He had a background of hypertension, hypercholesterolemia and was a heavy smoker. Biochemistry results showed raised white cell count of 28 × 109/L, elevated creatinine of 130 μmol/L, and venous lactate of 4.7 mmol/L.
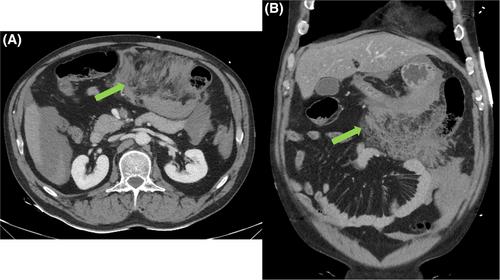
Computed tomography (CT) of the abdomen demonstrated a hematoma contained within the lesser sac (Figure 1A). Computed tomography angiography (CTA) revealed an abrupt cutoff of the first branch of superior mesenteric artery (SMA) at the site of hemorrhage suggesting dissection with a distal nonocclusive thrombus (Figures 1B and 2). It was possible that the SMA dissection led to the hematoma within the lesser sac and had tamponade itself. Therefore, there was no active hemorrhage on the subsequent CTA. Given that he was hemodynamically stable with no signs of peritonism, he was managed nonoperatively. He was commenced on lifelong antiplatelet therapy. He had a follow-up CTA which was unremarkable. He remained clinically well.
Patients with isolated superior mesenteric artery dissection (ISMAD) are at risk of intestinal ischemia. Patients usually present with intractable abdominal pain. Other symptoms include diarrhea, nausea, and vomiting. Risk factors for ISMAD include atherosclerotic disease, hypertension, and abdominal aortic aneurysm.1 CTA is the gold standard for diagnosis. Other imaging modalities include ultrasound and magnetic resonance angiography.2
The management of ISMAD consists of initial resuscitation. Patients with no signs of hemodynamic instability or peritonism can be managed nonoperatively.3 Anticoagulation is the mainstay of nonoperative management. A systematic review and meta-analysis reported that the majority of patients were commenced on anticoagulation therapy.4 Antiplatelet therapy has also been used in stable ISMAD patients with success.5
Operative management options include surgical or endovascular revascularization. Bypass grafting is the most common surgical procedure. Other surgical methods include thrombectomy or ligation of a branch of SMA.4
In conclusion, ISMAD is a rare cause of abdominal pain and prompt treatment is vital due to the risk of intestinal ischemia.
The authors declare no conflicts of interest.
According to the Institutional Review Board (IRB), there is no need for IRB approval for an image review article. A written informed consent was obtained from the patient before starting and the authors followed the principles outlined in the WMA Declaration of Helsinki throughout the writing process.
期刊介绍:
Advances in Digestive Medicine is the official peer-reviewed journal of GEST, DEST and TASL. Missions of AIDM are to enhance the quality of patient care, to promote researches in gastroenterology, endoscopy and hepatology related fields, and to develop platforms for digestive science. Specific areas of interest are included, but not limited to: • Acid-related disease • Small intestinal disease • Digestive cancer • Diagnostic & therapeutic endoscopy • Enteral nutrition • Innovation in endoscopic technology • Functional GI • Hepatitis • GI images • Liver cirrhosis • Gut hormone • NASH • Helicobacter pylori • Cancer screening • IBD • Laparoscopic surgery • Infectious disease of digestive tract • Genetics and metabolic disorder • Microbiota • Regenerative medicine • Pancreaticobiliary disease • Guideline & consensus.

 求助内容:
求助内容: 应助结果提醒方式:
应助结果提醒方式:


