{"title":"Effectiveness of upadacitinib in Japanese patients with prurigo-type atopic dermatitis: Four cases report","authors":"Keiji Kosaka MD, Akihiko Uchiyama MD, PhD, Mai Ishikawa MD, Sei-ichiro Motegi MD, PhD","doi":"10.1002/cia2.12333","DOIUrl":null,"url":null,"abstract":"<p>Prurigo-type atopic dermatitis (AD) is an AD variant characterized by excoriated papules, indurated nodules, and intense itching associated with type 2 cytokine responses.<span><sup>1</sup></span> Recently, upadacitinib, an oral selective Janus kinase (JAK) 1 inhibitor, was found to be efficacious and safe in treating moderate-to-severe AD in patients aged >12 years in a clinical trial.<span><sup>2</sup></span> However, few reports have demonstrated evidence of upadacitinib in prurigo-type AD. Here, we present four Japanese patients with prurigo-type AD who received upadacitinib.</p><p>Our cases included two male and two female patients with moderate-to-severe AD (Table S1). The patients fulfilled the AD criteria.<span><sup>3</sup></span> Cases 3 and 4 were also confirmed AD pathologically. They were treated with 15 or 30 mg upadacitinib, topical corticosteroid, and moisturizers once a day. Case 1: a 49-year-old female with widespread areas of erythema, nodules, and itching on her legs (Figure 1A). We initiated 30 mg of upadacitinib. After 8 weeks, she achieved Eczema Area and Severity Index (EASI)-90 and was itch-free (Figure 1B). Case 2: a 50-year-old female. She applied corticosteroid ointments on her refractory nodules for decades (Figure 1C). She had difficulty throughout her life due to insomnia caused by itching. We initiated 30 mg of upadacitinib; she was pruritus-free after 2 weeks, achieving EASI-90 after 4 weeks (Figure 1D). Case 3: a 64-year-old male with multiple pruritic nodules on his trunk and extremities (Figure 1E). We first initiated 30 mg of upadacitinib for his severe itchiness. After 4 weeks, his skin lesions and itching improved noticeably. Thus, we decreased the upadacitinib dose to 15 mg. After 12 weeks, his skin lesions almost disappeared (Figure 1F). Case 4: a 66-year-old male. He had multiple nodules on his neck and arms, forming plaque (Figure 1G). Although we diagnosed him with severe AD, we prescribed 15 mg of upadacitinib because of his age. After 12 weeks, he achieved EASI-90, and his skin lesions almost disappeared (Figure 1H). No adverse events were observed in the patients.</p><p>Figure 1I–K shows the transition of EASI, patient-oriented eczema measure (POEM), and pruritus numerical rating scale (NRS). A rapid decrease was seen in all categories from baseline to Week 4, and this effectiveness lasted for 12 weeks. Thymus and activation-regulated chemokine and immunoglobulin E in the serum were decreased from baseline to Week 4; however, some cases increased at Week 12 (Figure 1L,M).</p><p>The effectiveness of dupilumab and baricitinib against prurigo-type AD was recently reported.<span><sup>4, 5</sup></span> Dupilumab showed a significantly lower achievement rate of EASI-50 at 2 months in the prurigo compared with the non-prurigo group.<span><sup>4</sup></span> These results indicate the importance of suppressing not only IL-4 and IL-13 but also other cytokines, including IL-31 and thymic stromal lymphopoietin, which can induce itchiness during prurigo-type AD treatment. Chronic pruritus occurs due to neural sensitization to pruritus and the development of a pruritus-scratching cycle.<span><sup>6</sup></span> Our cases (Figure 1K) and previous reports on baricitinib achieved NRS-Itch-50 in 4 weeks.<span><sup>5</sup></span> JAK inhibitors can lead to the early improvement of prurigo-type AD by strongly suppressing itching.</p><p>The authors declare no conflict of interest.</p><p>Approval of the research protocol: No human participant was involved in this study.</p><p>Informed Consent: Informed consent was obtained from the patient.</p><p>Registry and the Registration No.: N/A.</p><p>Animal Studies: N/A.</p>","PeriodicalId":15543,"journal":{"name":"Journal of Cutaneous Immunology and Allergy","volume":"6 6","pages":"262-263"},"PeriodicalIF":0.9000,"publicationDate":"2023-10-09","publicationTypes":"Journal Article","fieldsOfStudy":null,"isOpenAccess":false,"openAccessPdf":"https://onlinelibrary.wiley.com/doi/epdf/10.1002/cia2.12333","citationCount":"0","resultStr":null,"platform":"Semanticscholar","paperid":null,"PeriodicalName":"Journal of Cutaneous Immunology and Allergy","FirstCategoryId":"1085","ListUrlMain":"https://onlinelibrary.wiley.com/doi/10.1002/cia2.12333","RegionNum":0,"RegionCategory":null,"ArticlePicture":[],"TitleCN":null,"AbstractTextCN":null,"PMCID":null,"EPubDate":"","PubModel":"","JCR":"Q4","JCRName":"ALLERGY","Score":null,"Total":0}
引用次数: 0
Abstract
Prurigo-type atopic dermatitis (AD) is an AD variant characterized by excoriated papules, indurated nodules, and intense itching associated with type 2 cytokine responses.1 Recently, upadacitinib, an oral selective Janus kinase (JAK) 1 inhibitor, was found to be efficacious and safe in treating moderate-to-severe AD in patients aged >12 years in a clinical trial.2 However, few reports have demonstrated evidence of upadacitinib in prurigo-type AD. Here, we present four Japanese patients with prurigo-type AD who received upadacitinib.
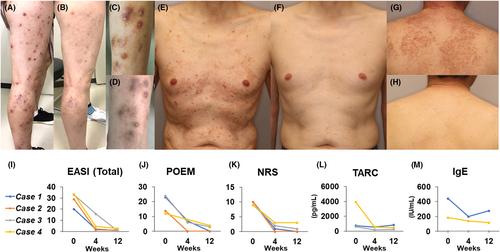
Our cases included two male and two female patients with moderate-to-severe AD (Table S1). The patients fulfilled the AD criteria.3 Cases 3 and 4 were also confirmed AD pathologically. They were treated with 15 or 30 mg upadacitinib, topical corticosteroid, and moisturizers once a day. Case 1: a 49-year-old female with widespread areas of erythema, nodules, and itching on her legs (Figure 1A). We initiated 30 mg of upadacitinib. After 8 weeks, she achieved Eczema Area and Severity Index (EASI)-90 and was itch-free (Figure 1B). Case 2: a 50-year-old female. She applied corticosteroid ointments on her refractory nodules for decades (Figure 1C). She had difficulty throughout her life due to insomnia caused by itching. We initiated 30 mg of upadacitinib; she was pruritus-free after 2 weeks, achieving EASI-90 after 4 weeks (Figure 1D). Case 3: a 64-year-old male with multiple pruritic nodules on his trunk and extremities (Figure 1E). We first initiated 30 mg of upadacitinib for his severe itchiness. After 4 weeks, his skin lesions and itching improved noticeably. Thus, we decreased the upadacitinib dose to 15 mg. After 12 weeks, his skin lesions almost disappeared (Figure 1F). Case 4: a 66-year-old male. He had multiple nodules on his neck and arms, forming plaque (Figure 1G). Although we diagnosed him with severe AD, we prescribed 15 mg of upadacitinib because of his age. After 12 weeks, he achieved EASI-90, and his skin lesions almost disappeared (Figure 1H). No adverse events were observed in the patients.
Figure 1I–K shows the transition of EASI, patient-oriented eczema measure (POEM), and pruritus numerical rating scale (NRS). A rapid decrease was seen in all categories from baseline to Week 4, and this effectiveness lasted for 12 weeks. Thymus and activation-regulated chemokine and immunoglobulin E in the serum were decreased from baseline to Week 4; however, some cases increased at Week 12 (Figure 1L,M).
The effectiveness of dupilumab and baricitinib against prurigo-type AD was recently reported.4, 5 Dupilumab showed a significantly lower achievement rate of EASI-50 at 2 months in the prurigo compared with the non-prurigo group.4 These results indicate the importance of suppressing not only IL-4 and IL-13 but also other cytokines, including IL-31 and thymic stromal lymphopoietin, which can induce itchiness during prurigo-type AD treatment. Chronic pruritus occurs due to neural sensitization to pruritus and the development of a pruritus-scratching cycle.6 Our cases (Figure 1K) and previous reports on baricitinib achieved NRS-Itch-50 in 4 weeks.5 JAK inhibitors can lead to the early improvement of prurigo-type AD by strongly suppressing itching.
The authors declare no conflict of interest.
Approval of the research protocol: No human participant was involved in this study.
Informed Consent: Informed consent was obtained from the patient.

 求助内容:
求助内容: 应助结果提醒方式:
应助结果提醒方式:


