Arthur W E Lieveld, Micah L A Heldeweg, Jasper Schouwenburg, Lars Veldhuis, Mark E Haaksma, Rutger M van Haaften, Berend P Teunissen, Jasper M Smit, Jos Twisk, Leo Heunks, Prabath W B Nanayakkara, Pieter Roel Tuinman
{"title":"Monitoring of pulmonary involvement in critically ill COVID-19 patients - should lung ultrasound be preferred over CT?","authors":"Arthur W E Lieveld, Micah L A Heldeweg, Jasper Schouwenburg, Lars Veldhuis, Mark E Haaksma, Rutger M van Haaften, Berend P Teunissen, Jasper M Smit, Jos Twisk, Leo Heunks, Prabath W B Nanayakkara, Pieter Roel Tuinman","doi":"10.1186/s13089-022-00299-x","DOIUrl":null,"url":null,"abstract":"<p><strong>Background: </strong>It is unclear if relevant changes in pulmonary involvement in critically ill COVID-19 patients can be reliably detected by the CT severity score (CTSS) and lung ultrasound score (LUSS), or if these changes have prognostic implications. In addition, it has been argued that adding pleural abnormalities to the LUSS could improve its prognostic value. The objective of this study was to compare LUSS and CTSS for the monitoring of COVID-19 pulmonary involvement through: first, establishing the correlation of LUSS (± pleural abnormalities) and CTSS throughout admission; second, assessing agreement and measurement error between raters for LUSS, pleural abnormalities, and CTSS; third, evaluating the association of the LUSS (± pleural abnormalities) and CTSS with mortality at different timepoints.</p><p><strong>Methods: </strong>This is a prospective, observational study, conducted during the second COVID-19 wave at the AmsterdamUMC, location VUmc. Adult COVID-19 ICU patients were prospectively included when a CT or a 12-zone LUS was performed at admission or at weekly intervals according to local protocol. Patients were followed 90 days or until death. We calculated the: (1) Correlation of the LUSS (± pleural abnormalities) and CTSS throughout admission with mixed models; (2) Intra-class correlation coefficients (ICCs) and smallest detectable changes (SDCs) between raters; (3) Association between the LUSS (± pleural abnormalities) and CTSS with mixed models.</p><p><strong>Results: </strong>82 consecutive patients were included. Correlation between LUSS and CTSS was 0.45 (95% CI 0.31-0.59). ICCs for LUSS, pleural abnormalities, and CTSS were 0.88 (95% CI 0.73-0.95), 0.94 (95% CI 0.90-0.96), and 0.84 (95% CI 0.65-0.93), with SDCs of 4.8, 1.4, and 3.9. The LUSS was associated with mortality in week 2, with a score difference between patients who survived or died greater than its SDC. Addition of pleural abnormalities was not beneficial. The CTSS was associated with mortality only in week 1, but with a score difference less than its SDC.</p><p><strong>Conclusions: </strong>LUSS correlated with CTSS throughout ICU admission but performed similar or better at agreement between raters and mortality prognostication. Given the benefits of LUS over CT, it should be preferred as initial monitoring tool.</p>","PeriodicalId":75201,"journal":{"name":"","volume":"15 1","pages":"11"},"PeriodicalIF":0.0,"publicationDate":"2023-02-26","publicationTypes":"Journal Article","fieldsOfStudy":null,"isOpenAccess":false,"openAccessPdf":"https://www.ncbi.nlm.nih.gov/pmc/articles/PMC9968403/pdf/","citationCount":"1","resultStr":null,"platform":"Semanticscholar","paperid":null,"PeriodicalName":"","FirstCategoryId":"1085","ListUrlMain":"https://doi.org/10.1186/s13089-022-00299-x","RegionNum":0,"RegionCategory":null,"ArticlePicture":[],"TitleCN":null,"AbstractTextCN":null,"PMCID":null,"EPubDate":"","PubModel":"","JCR":"","JCRName":"","Score":null,"Total":0}
引用次数: 1
Abstract
Background: It is unclear if relevant changes in pulmonary involvement in critically ill COVID-19 patients can be reliably detected by the CT severity score (CTSS) and lung ultrasound score (LUSS), or if these changes have prognostic implications. In addition, it has been argued that adding pleural abnormalities to the LUSS could improve its prognostic value. The objective of this study was to compare LUSS and CTSS for the monitoring of COVID-19 pulmonary involvement through: first, establishing the correlation of LUSS (± pleural abnormalities) and CTSS throughout admission; second, assessing agreement and measurement error between raters for LUSS, pleural abnormalities, and CTSS; third, evaluating the association of the LUSS (± pleural abnormalities) and CTSS with mortality at different timepoints.
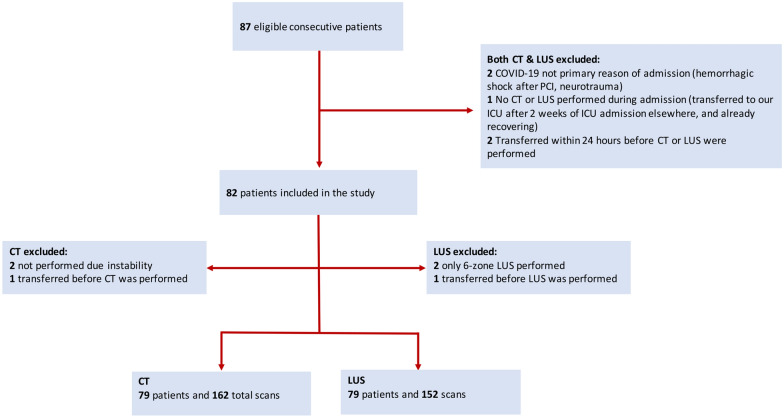
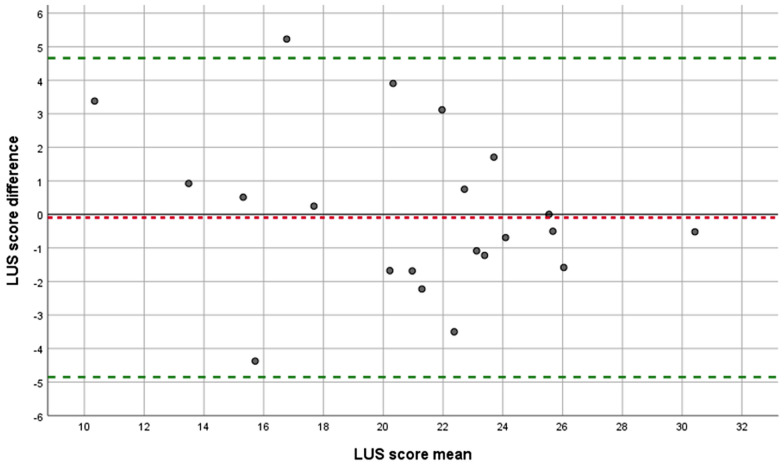
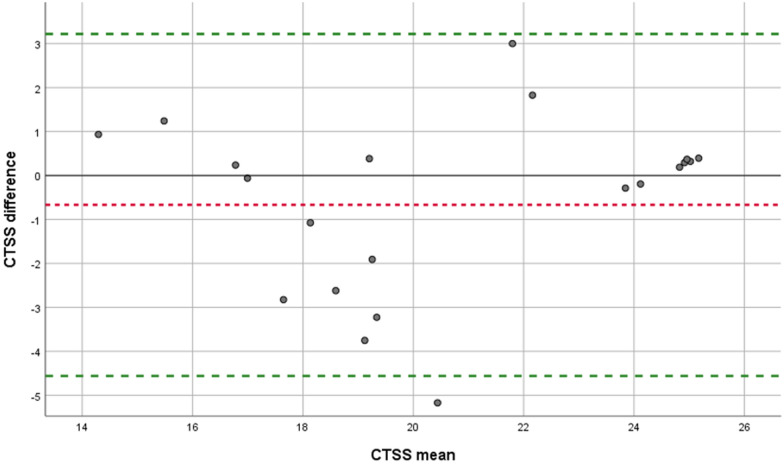
Methods: This is a prospective, observational study, conducted during the second COVID-19 wave at the AmsterdamUMC, location VUmc. Adult COVID-19 ICU patients were prospectively included when a CT or a 12-zone LUS was performed at admission or at weekly intervals according to local protocol. Patients were followed 90 days or until death. We calculated the: (1) Correlation of the LUSS (± pleural abnormalities) and CTSS throughout admission with mixed models; (2) Intra-class correlation coefficients (ICCs) and smallest detectable changes (SDCs) between raters; (3) Association between the LUSS (± pleural abnormalities) and CTSS with mixed models.
Results: 82 consecutive patients were included. Correlation between LUSS and CTSS was 0.45 (95% CI 0.31-0.59). ICCs for LUSS, pleural abnormalities, and CTSS were 0.88 (95% CI 0.73-0.95), 0.94 (95% CI 0.90-0.96), and 0.84 (95% CI 0.65-0.93), with SDCs of 4.8, 1.4, and 3.9. The LUSS was associated with mortality in week 2, with a score difference between patients who survived or died greater than its SDC. Addition of pleural abnormalities was not beneficial. The CTSS was associated with mortality only in week 1, but with a score difference less than its SDC.
Conclusions: LUSS correlated with CTSS throughout ICU admission but performed similar or better at agreement between raters and mortality prognostication. Given the benefits of LUS over CT, it should be preferred as initial monitoring tool.
背景:目前尚不清楚重症COVID-19患者肺部受累的相关变化是否可以通过CT严重程度评分(CTSS)和肺超声评分(LUSS)可靠地检测到,或者这些变化是否具有预后意义。此外,也有人认为在LUSS中加入胸膜异常可以提高其预后价值。本研究的目的是通过以下方式比较LUSS和CTSS对COVID-19肺部累及的监测:首先,建立入院期间LUSS(±胸膜异常)与CTSS的相关性;第二,评估LUSS、胸膜异常和CTSS评分者之间的一致性和测量误差;第三,评估LUSS(±胸膜异常)和CTSS与不同时间点死亡率的关系。方法:这是一项前瞻性观察性研究,于第二波COVID-19期间在阿姆斯特丹umc进行。根据当地方案,在入院时或每隔一周进行CT或12区LUS检查时,前瞻性纳入成年COVID-19 ICU患者。随访90天或至患者死亡。我们计算:(1)采用混合模型计算入院期间LUSS(±胸膜异常)与CTSS的相关性;(2)评分者的类内相关系数(ICCs)和最小可检测变化(SDCs);(3)混合模型下LUSS(±胸膜异常)与CTSS的关系。结果:连续纳入82例患者。LUSS与CTSS的相关性为0.45 (95% CI 0.31-0.59)。LUSS、胸膜异常和CTSS的ICCs分别为0.88 (95% CI 0.73-0.95)、0.94 (95% CI 0.90-0.96)和0.84 (95% CI 0.65-0.93), SDCs分别为4.8、1.4和3.9。LUSS与第2周的死亡率相关,存活或死亡患者之间的评分差异大于其SDC。增加胸膜异常是不利的。CTSS仅在第1周与死亡率相关,但评分差异小于其SDC。结论:在ICU住院期间,LUSS与CTSS相关,但在评分者和死亡率预测之间的一致性相似或更好。考虑到LUS相对于CT的优势,它应该是首选的初始监测工具。
 求助内容:
求助内容: 应助结果提醒方式:
应助结果提醒方式:


