Khi Yung Fong, Joseph Jonathan Zhao, Rehena Sultana, Joycelyn Jie Xin Lee, Suat Ying Lee, Stephen Lam Chan, Thomas Yau, David Wai Meng Tai, Raghav Sundar, Chow Wei Too
{"title":"First-Line Systemic Therapies for Advanced Hepatocellular Carcinoma: A Systematic Review and Patient-Level Network Meta-Analysis.","authors":"Khi Yung Fong, Joseph Jonathan Zhao, Rehena Sultana, Joycelyn Jie Xin Lee, Suat Ying Lee, Stephen Lam Chan, Thomas Yau, David Wai Meng Tai, Raghav Sundar, Chow Wei Too","doi":"10.1159/000526639","DOIUrl":null,"url":null,"abstract":"<p><strong>Introduction: </strong>Sorafenib was historically the standard of care for advanced hepatocellular carcinoma (aHCC) until it was superseded by the combination of atezolizumab and bevacizumab. Thereafter, several novel first-line combination therapies have demonstrated favorable outcomes. The efficacies of these treatments in relation to current and previous standards of care are unknown, necessitating an overarching evaluation.</p><p><strong>Methods: </strong>A systematic literature search was conducted on PubMed, EMBASE, Scopus, and the Cochrane Controlled Register of Trials for phase III randomized controlled trials investigating first-line systemic therapies for aHCC. Kaplan-Meier curves for overall survival (OS) and progression-free survival (PFS) were graphically reconstructed to retrieve individual patient-level data. Derived hazard ratios (HRs) for each study were pooled in a random-effects network meta-analysis (NMA). NMAs were also conducted using study-level HRs for various subgroups, according to viral etiology, Barcelona Clinic Liver Cancer (BCLC) staging, alpha-fetoprotein (AFP) levels, macrovascular invasion, and extrahepatic spread. Treatment strategies were ranked using <i>p</i> scores.</p><p><strong>Results: </strong>Among 4,321 articles identified, 12 trials and 9,589 patients were included for analysis. Only two therapies showed OS benefit over sorafenib: combined anti-programmed-death and anti-VEGF pathway inhibitor monoclonal antibodies (Anti-PD-(L)1/VEGF Ab), including atezolizumab-bevacizumab and sintilimab-bevacizumab biosimilar (HR = 0.63, 95% CI = 0.53-0.76) and tremelimumab-durvalumab (HR = 0.78, 95% CI = 0.66-0.92). Anti-PD-(L)1/VEGF Ab showed OS benefit over all other therapies except tremelimumab-durvalumab. Low heterogeneity (<i>I</i><sup>2</sup> = 0%) and inconsistency (Cochran's <i>Q</i> = 0.52, <i>p</i> = 0.773) was observed. <i>p</i> scores for OS ranked Anti-PD-(L)1/VEGF Ab as the best treatment in all subgroups, except hepatitis B where atezolizumab-cabozantinib ranked highest for both OS and PFS, as well as nonviral HCC and AFP ≥400 μg/L where tremelimumab-durvalumab ranked highest for OS.</p><p><strong>Conclusion: </strong>This NMA supports Anti-PD-(L)1/VEGF Ab as the first-line therapy for aHCC and demonstrates a comparable benefit for tremelimumab-durvalumab which also extends to certain subgroups. Results of the subgroup analysis may guide treatment according to baseline characteristics, while pending further studies.</p>","PeriodicalId":18156,"journal":{"name":"Liver Cancer","volume":"12 1","pages":"7-18"},"PeriodicalIF":11.6000,"publicationDate":"2022-08-23","publicationTypes":"Journal Article","fieldsOfStudy":null,"isOpenAccess":false,"openAccessPdf":"https://ftp.ncbi.nlm.nih.gov/pub/pmc/oa_pdf/76/47/lic-0012-0007.PMC9982345.pdf","citationCount":"0","resultStr":null,"platform":"Semanticscholar","paperid":null,"PeriodicalName":"Liver Cancer","FirstCategoryId":"3","ListUrlMain":"https://doi.org/10.1159/000526639","RegionNum":1,"RegionCategory":"医学","ArticlePicture":[],"TitleCN":null,"AbstractTextCN":null,"PMCID":null,"EPubDate":"2023/2/1 0:00:00","PubModel":"eCollection","JCR":"Q1","JCRName":"GASTROENTEROLOGY & HEPATOLOGY","Score":null,"Total":0}
引用次数: 0
Abstract
Introduction: Sorafenib was historically the standard of care for advanced hepatocellular carcinoma (aHCC) until it was superseded by the combination of atezolizumab and bevacizumab. Thereafter, several novel first-line combination therapies have demonstrated favorable outcomes. The efficacies of these treatments in relation to current and previous standards of care are unknown, necessitating an overarching evaluation.
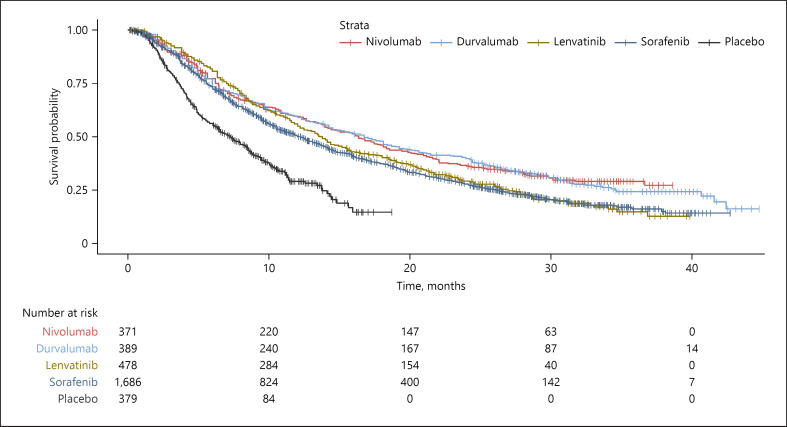
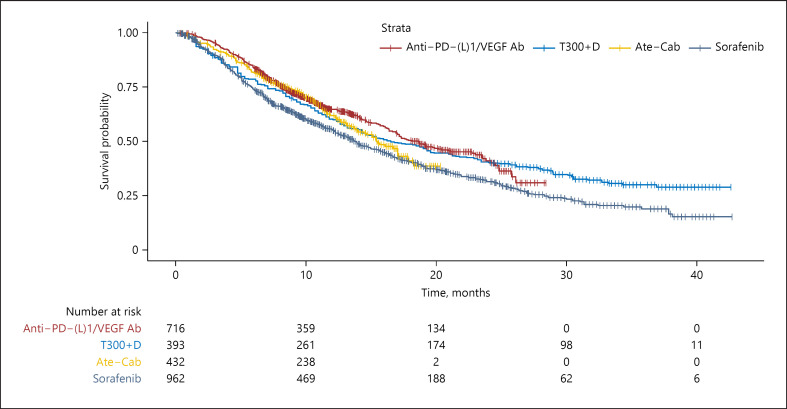
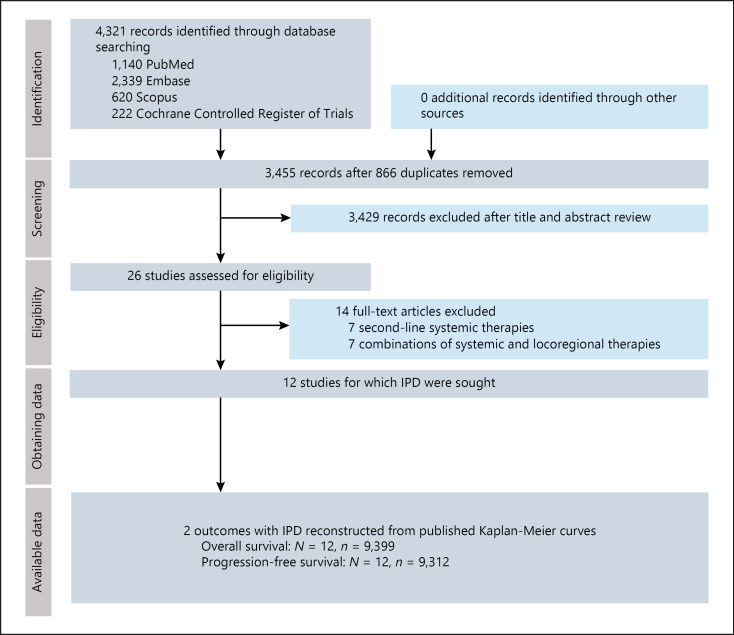
Methods: A systematic literature search was conducted on PubMed, EMBASE, Scopus, and the Cochrane Controlled Register of Trials for phase III randomized controlled trials investigating first-line systemic therapies for aHCC. Kaplan-Meier curves for overall survival (OS) and progression-free survival (PFS) were graphically reconstructed to retrieve individual patient-level data. Derived hazard ratios (HRs) for each study were pooled in a random-effects network meta-analysis (NMA). NMAs were also conducted using study-level HRs for various subgroups, according to viral etiology, Barcelona Clinic Liver Cancer (BCLC) staging, alpha-fetoprotein (AFP) levels, macrovascular invasion, and extrahepatic spread. Treatment strategies were ranked using p scores.
Results: Among 4,321 articles identified, 12 trials and 9,589 patients were included for analysis. Only two therapies showed OS benefit over sorafenib: combined anti-programmed-death and anti-VEGF pathway inhibitor monoclonal antibodies (Anti-PD-(L)1/VEGF Ab), including atezolizumab-bevacizumab and sintilimab-bevacizumab biosimilar (HR = 0.63, 95% CI = 0.53-0.76) and tremelimumab-durvalumab (HR = 0.78, 95% CI = 0.66-0.92). Anti-PD-(L)1/VEGF Ab showed OS benefit over all other therapies except tremelimumab-durvalumab. Low heterogeneity (I2 = 0%) and inconsistency (Cochran's Q = 0.52, p = 0.773) was observed. p scores for OS ranked Anti-PD-(L)1/VEGF Ab as the best treatment in all subgroups, except hepatitis B where atezolizumab-cabozantinib ranked highest for both OS and PFS, as well as nonviral HCC and AFP ≥400 μg/L where tremelimumab-durvalumab ranked highest for OS.
Conclusion: This NMA supports Anti-PD-(L)1/VEGF Ab as the first-line therapy for aHCC and demonstrates a comparable benefit for tremelimumab-durvalumab which also extends to certain subgroups. Results of the subgroup analysis may guide treatment according to baseline characteristics, while pending further studies.
期刊介绍:
Liver Cancer is a journal that serves the international community of researchers and clinicians by providing a platform for research results related to the causes, mechanisms, and therapy of liver cancer. It focuses on molecular carcinogenesis, prevention, surveillance, diagnosis, and treatment, including molecular targeted therapy. The journal publishes clinical and translational research in the field of liver cancer in both humans and experimental models. It publishes original and review articles and has an Impact Factor of 13.8. The journal is indexed and abstracted in various platforms including PubMed, PubMed Central, Web of Science, Science Citation Index, Science Citation Index Expanded, Google Scholar, DOAJ, Chemical Abstracts Service, Scopus, Embase, Pathway Studio, and WorldCat.
 求助内容:
求助内容: 应助结果提醒方式:
应助结果提醒方式:


