{"title":"[Use of metformin in patients with type 2 diabetes and acute myocardial infarction: safety and impact on glycemic control].","authors":"M A Korotina, I G Pochinka, L G Strongin","doi":"10.14341/probl13170","DOIUrl":null,"url":null,"abstract":"<p><strong>Background: </strong>Myocardial infarction (MI) in patients with diabetes type 2 (T2DM) occurs 1.5-3.0 times higher than in general population. Metformin is contraindicated for patients with T2DM and acute coronary syndrome due to the risk of developing lactic acidosis. Using metformin more than 48 hours of MI is a topical question, which will help to improve patient's safety.</p><p><strong>Aim: </strong>To evaluate the safety and quality of glycemic control using metformin in patients with T2DM during inpatient treatment for MIMATERIALS AND METHODS: The study included 161 patients with T2DM, who were hospitalized consecutively with acute MI with ST-elevation and underwent percutaneous coronary intervention (PCI). Average time of metformin initiation was 5th day from admission. Creatinine was assessed at admission and 48 hours after PCI. The acid-base balance and lactate were assessed at admission and on the 3rd day after the start of using metformin. Criteria for the effectiveness of glycemic control was the proportion of glycemic measurements in target range of 6.1-10.0 mmol/l during hospitalization (\"hospital time in range\", hTIR). hTIR >55% was considered to be a critical level. The long-term outcome was estimated at 365 days after hospitalization.</p><p><strong>Results: </strong>Metformin was prescribed to 99 patients (61%) (\"M+\"group) during the hospitalization, 62 patients were in \"M-\"group. Use of metformin was accompanied with better glycemic control in the «M+» group compared to the «M-»: mean glycemia 9.3 ± 1.6 vs 10.3 ± 2.3 mmol/l (p=0,002), SD 2.87 ± 1.1 vs 3.26 ± 1.8 (p=0,049), hTIR 60 ± 18% vs 48 ± 23% (p<0,001). There were clinically insignificant changes in acid-base balance on the 3rd day from the start of metformin use in the \"M+\" group, the lactate level did not increase. Use of metformin before to hospitalization with MI was not associated with an increased risk of developing acute kidney injury (AKI): RR 0.85 (0.37-1.96), p=0,691.</p><p><strong>Conclusion: </strong>Use of metformin in patients with T2DM and acute MI is associated with better glycemic control. Carrying out angiography in patients, treated with metformin before the hospitalization, is not accompanied by an increased risk of developing AKI. Appointment of metformin in 3-7 days after angiography does not lead to an increase level of lactate and significant deviations in acid-base balance.</p>","PeriodicalId":20433,"journal":{"name":"Problemy endokrinologii","volume":"69 1","pages":"28-35"},"PeriodicalIF":0.0000,"publicationDate":"2023-02-25","publicationTypes":"Journal Article","fieldsOfStudy":null,"isOpenAccess":false,"openAccessPdf":"https://www.ncbi.nlm.nih.gov/pmc/articles/PMC9978873/pdf/","citationCount":"0","resultStr":null,"platform":"Semanticscholar","paperid":null,"PeriodicalName":"Problemy endokrinologii","FirstCategoryId":"1085","ListUrlMain":"https://doi.org/10.14341/probl13170","RegionNum":0,"RegionCategory":null,"ArticlePicture":[],"TitleCN":null,"AbstractTextCN":null,"PMCID":null,"EPubDate":"","PubModel":"","JCR":"Q4","JCRName":"Medicine","Score":null,"Total":0}
引用次数: 0
Abstract
Background: Myocardial infarction (MI) in patients with diabetes type 2 (T2DM) occurs 1.5-3.0 times higher than in general population. Metformin is contraindicated for patients with T2DM and acute coronary syndrome due to the risk of developing lactic acidosis. Using metformin more than 48 hours of MI is a topical question, which will help to improve patient's safety.
Aim: To evaluate the safety and quality of glycemic control using metformin in patients with T2DM during inpatient treatment for MIMATERIALS AND METHODS: The study included 161 patients with T2DM, who were hospitalized consecutively with acute MI with ST-elevation and underwent percutaneous coronary intervention (PCI). Average time of metformin initiation was 5th day from admission. Creatinine was assessed at admission and 48 hours after PCI. The acid-base balance and lactate were assessed at admission and on the 3rd day after the start of using metformin. Criteria for the effectiveness of glycemic control was the proportion of glycemic measurements in target range of 6.1-10.0 mmol/l during hospitalization ("hospital time in range", hTIR). hTIR >55% was considered to be a critical level. The long-term outcome was estimated at 365 days after hospitalization.
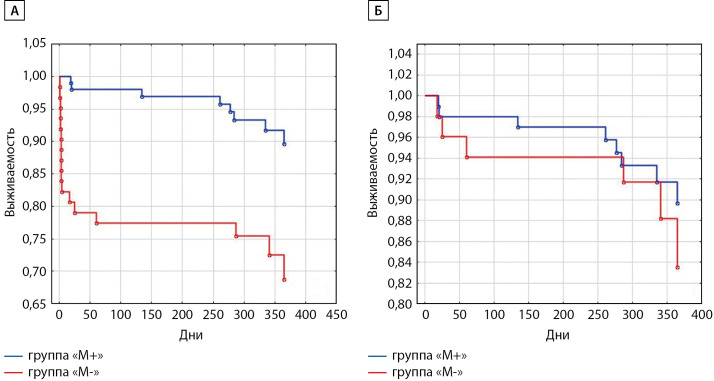
Results: Metformin was prescribed to 99 patients (61%) ("M+"group) during the hospitalization, 62 patients were in "M-"group. Use of metformin was accompanied with better glycemic control in the «M+» group compared to the «M-»: mean glycemia 9.3 ± 1.6 vs 10.3 ± 2.3 mmol/l (p=0,002), SD 2.87 ± 1.1 vs 3.26 ± 1.8 (p=0,049), hTIR 60 ± 18% vs 48 ± 23% (p<0,001). There were clinically insignificant changes in acid-base balance on the 3rd day from the start of metformin use in the "M+" group, the lactate level did not increase. Use of metformin before to hospitalization with MI was not associated with an increased risk of developing acute kidney injury (AKI): RR 0.85 (0.37-1.96), p=0,691.
Conclusion: Use of metformin in patients with T2DM and acute MI is associated with better glycemic control. Carrying out angiography in patients, treated with metformin before the hospitalization, is not accompanied by an increased risk of developing AKI. Appointment of metformin in 3-7 days after angiography does not lead to an increase level of lactate and significant deviations in acid-base balance.
期刊介绍:
Since 1955 the “Problems of Endocrinology” (or “Problemy Endocrinologii”) Journal publishes timely articles, balancing both clinical and experimental research, case reports, reviews and lectures on pressing problems of endocrinology. The Journal is aimed to the most topical issues of endocrinology: to chemical structure, biosynthesis and metabolism of hormones, the mechanism of their action at cellular and molecular level; pathogenesis and to clinic of the endocrine diseases, new methods of their diagnostics and treatment. The Journal: features original national and foreign research articles, reflecting world endocrinology development; issues thematic editions on specific areas; publishes chronicle of major international congress sessions and workshops on endocrinology, as well as state-of-the-art guidelines; is intended for scientists, endocrinologists diabetologists and specialists of allied trade, general practitioners, family physicians and pediatrics.

 求助内容:
求助内容: 应助结果提醒方式:
应助结果提醒方式:


