{"title":"Comparison of Four Intrapartum Cardiotocography Classifications for Predicting Neonatal Acidemia at Birth.","authors":"Nika Troha, Katja Razem, Ursa Luzovec, Miha Lucovnik","doi":"10.1155/2023/5853889","DOIUrl":null,"url":null,"abstract":"<p><strong>Objective: </strong>To compare diagnostic values of four intrapartum cardiotocography (CTG) classifications in predicting neonatal acidemia at birth.</p><p><strong>Methods: </strong>Retrospective case-control study. Forty-three CTG traces with an umbilical artery pH < 7.00 (study group) and 43 traces with a pH ≥ 7.00 (control group) were analyzed. Inclusion criteria were singleton pregnancy, cephalic presentation, admission to labour ward during active phase of first stage of labour, and gestational age 37<sup>+0</sup> to 41<sup>+6</sup> weeks. Exclusion criteria were suspected intrauterine growth restriction, oligohydramnios, polyhydramnios, pregestational or gestational insulin-dependent diabetes mellitus, and preeclampsia. Last 30-60 minutes before delivery of CTG traces was classified retrospectively according to four classification systems-International Federation of Gynecology and Obstetrics (FIGO), Royal College of Obstetricians and Gynaecologists (RCOG), National Institute of Child Health and Human Development (NICHD), and the 5-tier system by Parer and Ikeda. Predictive value of each classification for neonatal acidemia was assessed using receiver operating characteristics (ROC) analysis.</p><p><strong>Results: </strong>FIGO, RCOG, and NICHD classifications predicted neonatal acidemia with areas under the ROC curves (AUC) of 0.73, 95% confidence interval (CI) 0.63-0.84; 0.72, 95% CI 0.60-0.83; and 0.69, 95% CI 0.57-0.80, respectively. The five-tier system by Parer and Ikeda had significantly better predictive value with an AUC of 0.96, 95% CI 0.91-1.00.</p><p><strong>Conclusions: </strong>The 5-tier classification system proposed by Parer and Ikeda for assessing CTG in labour was superior to FIGO, RCOG, and NICHD intrapartum CTG classifications in predicting severe neonatal acidemia at birth.</p>","PeriodicalId":47062,"journal":{"name":"Journal of Pregnancy","volume":"2023 ","pages":"5853889"},"PeriodicalIF":2.2000,"publicationDate":"2023-02-13","publicationTypes":"Journal Article","fieldsOfStudy":null,"isOpenAccess":false,"openAccessPdf":"https://www.ncbi.nlm.nih.gov/pmc/articles/PMC9940944/pdf/","citationCount":"0","resultStr":null,"platform":"Semanticscholar","paperid":null,"PeriodicalName":"Journal of Pregnancy","FirstCategoryId":"1085","ListUrlMain":"https://doi.org/10.1155/2023/5853889","RegionNum":0,"RegionCategory":null,"ArticlePicture":[],"TitleCN":null,"AbstractTextCN":null,"PMCID":null,"EPubDate":"2023/1/1 0:00:00","PubModel":"eCollection","JCR":"Q1","JCRName":"OBSTETRICS & GYNECOLOGY","Score":null,"Total":0}
引用次数: 0
Abstract
Objective: To compare diagnostic values of four intrapartum cardiotocography (CTG) classifications in predicting neonatal acidemia at birth.
Methods: Retrospective case-control study. Forty-three CTG traces with an umbilical artery pH < 7.00 (study group) and 43 traces with a pH ≥ 7.00 (control group) were analyzed. Inclusion criteria were singleton pregnancy, cephalic presentation, admission to labour ward during active phase of first stage of labour, and gestational age 37+0 to 41+6 weeks. Exclusion criteria were suspected intrauterine growth restriction, oligohydramnios, polyhydramnios, pregestational or gestational insulin-dependent diabetes mellitus, and preeclampsia. Last 30-60 minutes before delivery of CTG traces was classified retrospectively according to four classification systems-International Federation of Gynecology and Obstetrics (FIGO), Royal College of Obstetricians and Gynaecologists (RCOG), National Institute of Child Health and Human Development (NICHD), and the 5-tier system by Parer and Ikeda. Predictive value of each classification for neonatal acidemia was assessed using receiver operating characteristics (ROC) analysis.
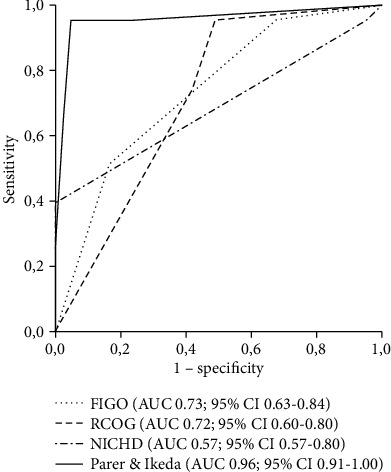
Results: FIGO, RCOG, and NICHD classifications predicted neonatal acidemia with areas under the ROC curves (AUC) of 0.73, 95% confidence interval (CI) 0.63-0.84; 0.72, 95% CI 0.60-0.83; and 0.69, 95% CI 0.57-0.80, respectively. The five-tier system by Parer and Ikeda had significantly better predictive value with an AUC of 0.96, 95% CI 0.91-1.00.
Conclusions: The 5-tier classification system proposed by Parer and Ikeda for assessing CTG in labour was superior to FIGO, RCOG, and NICHD intrapartum CTG classifications in predicting severe neonatal acidemia at birth.
期刊介绍:
Journal of Pregnancy is a peer-reviewed, Open Access journal that publishes original research articles, review articles, and clinical studies related to all aspects of pregnancy and childbirth. The journal welcomes submissions on breastfeeding, labor, maternal health and the biomedical aspects of pregnancy.

 求助内容:
求助内容: 应助结果提醒方式:
应助结果提醒方式:


