A Neural Network Model Using Pain Score Patterns to Predict the Need for Outpatient Opioid Refills Following Ambulatory Surgery: Algorithm Development and Validation.
Rodney Allanigue Gabriel, Sierra Simpson, William Zhong, Brittany Nicole Burton, Soraya Mehdipour, Engy Tadros Said
{"title":"A Neural Network Model Using Pain Score Patterns to Predict the Need for Outpatient Opioid Refills Following Ambulatory Surgery: Algorithm Development and Validation.","authors":"Rodney Allanigue Gabriel, Sierra Simpson, William Zhong, Brittany Nicole Burton, Soraya Mehdipour, Engy Tadros Said","doi":"10.2196/40455","DOIUrl":null,"url":null,"abstract":"<p><strong>Background: </strong>Expansion of clinical guidance tools is crucial to identify patients at risk of requiring an opioid refill after outpatient surgery.</p><p><strong>Objective: </strong>The objective of this study was to develop machine learning algorithms incorporating pain and opioid features to predict the need for outpatient opioid refills following ambulatory surgery.</p><p><strong>Methods: </strong>Neural networks, regression, random forest, and a support vector machine were used to evaluate the data set. For each model, oversampling and undersampling techniques were implemented to balance the data set. Hyperparameter tuning based on k-fold cross-validation was performed, and feature importance was ranked based on a Shapley Additive Explanations (SHAP) explainer model. To assess performance, we calculated the average area under the receiver operating characteristics curve (AUC), F1-score, sensitivity, and specificity for each model.</p><p><strong>Results: </strong>There were 1333 patients, of whom 144 (10.8%) refilled their opioid prescription within 2 weeks after outpatient surgery. The average AUC calculated from k-fold cross-validation was 0.71 for the neural network model. When the model was validated on the test set, the AUC was 0.75. The features with the highest impact on model output were performance of a regional nerve block, postanesthesia care unit maximum pain score, postanesthesia care unit median pain score, active smoking history, and total perioperative opioid consumption.</p><p><strong>Conclusions: </strong>Applying machine learning algorithms allows providers to better predict outcomes that require specialized health care resources such as transitional pain clinics. This model can aid as a clinical decision support for early identification of at-risk patients who may benefit from transitional pain clinic care perioperatively in ambulatory surgery.</p>","PeriodicalId":73557,"journal":{"name":"JMIR perioperative medicine","volume":"6 ","pages":"e40455"},"PeriodicalIF":0.0000,"publicationDate":"2023-02-08","publicationTypes":"Journal Article","fieldsOfStudy":null,"isOpenAccess":false,"openAccessPdf":"https://www.ncbi.nlm.nih.gov/pmc/articles/PMC9947767/pdf/","citationCount":"1","resultStr":null,"platform":"Semanticscholar","paperid":null,"PeriodicalName":"JMIR perioperative medicine","FirstCategoryId":"1085","ListUrlMain":"https://doi.org/10.2196/40455","RegionNum":0,"RegionCategory":null,"ArticlePicture":[],"TitleCN":null,"AbstractTextCN":null,"PMCID":null,"EPubDate":"","PubModel":"","JCR":"","JCRName":"","Score":null,"Total":0}
引用次数: 1
Abstract
Background: Expansion of clinical guidance tools is crucial to identify patients at risk of requiring an opioid refill after outpatient surgery.
Objective: The objective of this study was to develop machine learning algorithms incorporating pain and opioid features to predict the need for outpatient opioid refills following ambulatory surgery.
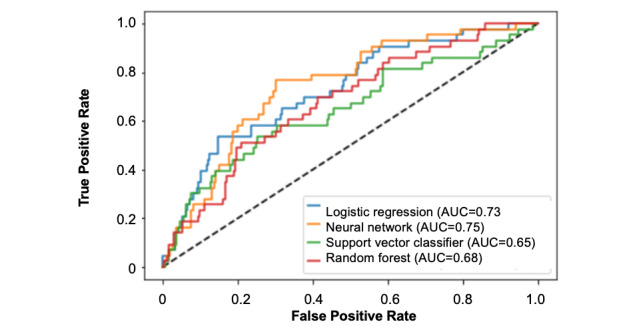
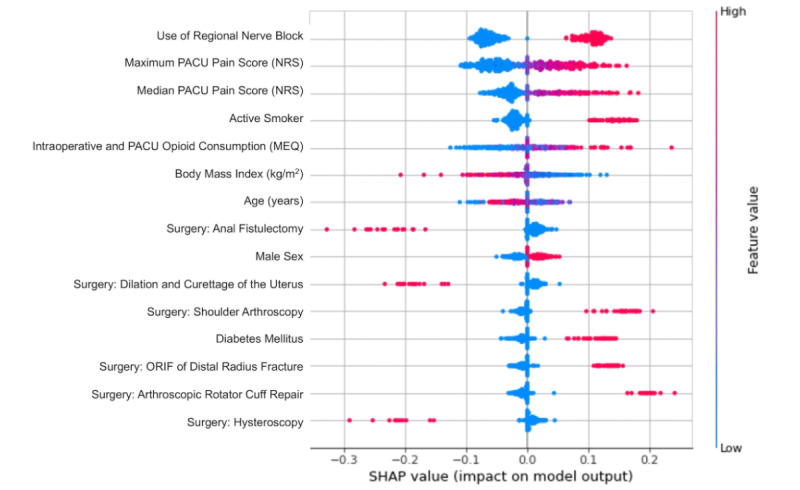
Methods: Neural networks, regression, random forest, and a support vector machine were used to evaluate the data set. For each model, oversampling and undersampling techniques were implemented to balance the data set. Hyperparameter tuning based on k-fold cross-validation was performed, and feature importance was ranked based on a Shapley Additive Explanations (SHAP) explainer model. To assess performance, we calculated the average area under the receiver operating characteristics curve (AUC), F1-score, sensitivity, and specificity for each model.
Results: There were 1333 patients, of whom 144 (10.8%) refilled their opioid prescription within 2 weeks after outpatient surgery. The average AUC calculated from k-fold cross-validation was 0.71 for the neural network model. When the model was validated on the test set, the AUC was 0.75. The features with the highest impact on model output were performance of a regional nerve block, postanesthesia care unit maximum pain score, postanesthesia care unit median pain score, active smoking history, and total perioperative opioid consumption.
Conclusions: Applying machine learning algorithms allows providers to better predict outcomes that require specialized health care resources such as transitional pain clinics. This model can aid as a clinical decision support for early identification of at-risk patients who may benefit from transitional pain clinic care perioperatively in ambulatory surgery.

 求助内容:
求助内容: 应助结果提醒方式:
应助结果提醒方式:


