Markian Bojko MD, MPH , Korri S. Hershenhouse MD , Ramsey S. Elsayed MD , Brittany Abt MD , Robbin G. Cohen MD. MMM , Raymond Lee MD , Michael E. Bowdish MD, MS , Vaughn A. Starnes MD
{"title":"Surgical Outcomes After Reconstruction of the Aortomitral Curtain","authors":"Markian Bojko MD, MPH , Korri S. Hershenhouse MD , Ramsey S. Elsayed MD , Brittany Abt MD , Robbin G. Cohen MD. MMM , Raymond Lee MD , Michael E. Bowdish MD, MS , Vaughn A. Starnes MD","doi":"10.1053/j.semtcvs.2022.11.008","DOIUrl":null,"url":null,"abstract":"<div><p><span><span>Repair of concomitant aortic and mitral valvular disease with involvement of the aortomitral curtain requires a technically complex operation colloquially termed the commando procedure. Surgical outcomes of this procedure are not well described. The objective of this study was to examine outcomes of the commando procedure at our center. We identified all patients undergoing concomitant aortic and </span>mitral valve replacements<span> from 2004–2021. Of 363 patients, 41 underwent reconstruction of the aortomitral curtain. Survival analysis and multivariable modeling were used to examine outcomes and risk factors for mortality. The median age was 52 (IQR 44-71) years. Preoperatively, 4 of 41 (9.8%) patients had renal failure, and 10 of 41 (24.4%) had a stroke. The most common surgical indication was endocarditis in 25 of 41 (61.0%) patients. 25 of 41 (61.0%) patients underwent redo </span></span>sternotomy<span><span>, and 23 of 41 (56.1%) had previous prosthetic valves<span><span>. Operative mortality was 14 of 41 (34.1%), and 8 of 41 (9.5%) patients received a </span>permanent pacemaker. Survival at 1, 3, and 5 years was 55.4% (95% confidence interval (CI), 40.6–75.5%), 50.3% (35.0–72.3%), and 37.7% (19.3–73.9%) respectively. Cox </span></span>proportional hazards regression identified previous sternotomy (HR 4.76, 95% CI 1.21–18.73), and female gender (HR 1.39, 95% CI 1.17–13.82) as risk factors for mortality. Patients undergoing reconstruction of the aortomitral curtain represent a high-risk population with complex surgical indications. Due to high perioperative morbidity and mortality, this procedure should be performed only when necessary. Despite a high up front morbidity burden, outcomes remain favorable for patients who survive the initial hospitalization.</span></p></div>","PeriodicalId":48592,"journal":{"name":"Seminars in Thoracic and Cardiovascular Surgery","volume":"36 2","pages":"Pages 158-166"},"PeriodicalIF":2.6000,"publicationDate":"2024-06-01","publicationTypes":"Journal Article","fieldsOfStudy":null,"isOpenAccess":false,"openAccessPdf":"","citationCount":"0","resultStr":null,"platform":"Semanticscholar","paperid":null,"PeriodicalName":"Seminars in Thoracic and Cardiovascular Surgery","FirstCategoryId":"3","ListUrlMain":"https://www.sciencedirect.com/science/article/pii/S1043067922002751","RegionNum":3,"RegionCategory":"医学","ArticlePicture":[],"TitleCN":null,"AbstractTextCN":null,"PMCID":null,"EPubDate":"","PubModel":"","JCR":"Q2","JCRName":"CARDIAC & CARDIOVASCULAR SYSTEMS","Score":null,"Total":0}
引用次数: 0
Abstract
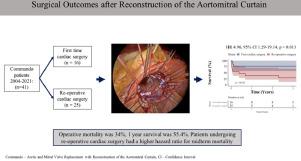
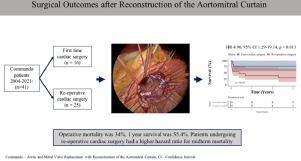
Repair of concomitant aortic and mitral valvular disease with involvement of the aortomitral curtain requires a technically complex operation colloquially termed the commando procedure. Surgical outcomes of this procedure are not well described. The objective of this study was to examine outcomes of the commando procedure at our center. We identified all patients undergoing concomitant aortic and mitral valve replacements from 2004–2021. Of 363 patients, 41 underwent reconstruction of the aortomitral curtain. Survival analysis and multivariable modeling were used to examine outcomes and risk factors for mortality. The median age was 52 (IQR 44-71) years. Preoperatively, 4 of 41 (9.8%) patients had renal failure, and 10 of 41 (24.4%) had a stroke. The most common surgical indication was endocarditis in 25 of 41 (61.0%) patients. 25 of 41 (61.0%) patients underwent redo sternotomy, and 23 of 41 (56.1%) had previous prosthetic valves. Operative mortality was 14 of 41 (34.1%), and 8 of 41 (9.5%) patients received a permanent pacemaker. Survival at 1, 3, and 5 years was 55.4% (95% confidence interval (CI), 40.6–75.5%), 50.3% (35.0–72.3%), and 37.7% (19.3–73.9%) respectively. Cox proportional hazards regression identified previous sternotomy (HR 4.76, 95% CI 1.21–18.73), and female gender (HR 1.39, 95% CI 1.17–13.82) as risk factors for mortality. Patients undergoing reconstruction of the aortomitral curtain represent a high-risk population with complex surgical indications. Due to high perioperative morbidity and mortality, this procedure should be performed only when necessary. Despite a high up front morbidity burden, outcomes remain favorable for patients who survive the initial hospitalization.
期刊介绍:
Seminars in Thoracic and Cardiovascular Surgery is devoted to providing a forum for cardiothoracic surgeons to disseminate and discuss important new information and to gain insight into unresolved areas of question in the specialty. Each issue presents readers with a selection of original peer-reviewed articles accompanied by editorial commentary from specialists in the field. In addition, readers are offered valuable invited articles: State of Views editorials and Current Readings highlighting the latest contributions on central or controversial issues. Another prized feature is expert roundtable discussions in which experts debate critical questions for cardiothoracic treatment and care. Seminars is an invitation-only publication that receives original submissions transferred ONLY from its sister publication, The Journal of Thoracic and Cardiovascular Surgery. As we continue to expand the reach of the Journal, we will explore the possibility of accepting unsolicited manuscripts in the future.

 求助内容:
求助内容: 应助结果提醒方式:
应助结果提醒方式:


