Adam Mayer, Alexandra Sperry, Laarni Quimson, Rennie L Rhee
{"title":"Long-Term Clinical and Radiographic Outcomes in Patients With Clinically Isolated Aortitis.","authors":"Adam Mayer, Alexandra Sperry, Laarni Quimson, Rennie L Rhee","doi":"10.1002/acr2.11504","DOIUrl":null,"url":null,"abstract":"<p><strong>Objective: </strong>The optimal management of patients with incidentally found clinically isolated aortitis (CIA) after aneurysm repair is unclear. This study compared long-term surgical and clinical outcomes after surgical repair of thoracic aortic aneurysm between patients with CIA and patients with noninflammatory etiologies.</p><p><strong>Methods: </strong>This is a matched cohort study. Patients with CIA were identified by histopathology following open thoracic aortic aneurysm repair. Two comparators without inflammation on pathology were matched to each patient by year of surgical repair. Outcomes included surgical complications, new vascular abnormalities on imaging, and death.</p><p><strong>Results: </strong>One hundred sixty-two patients were included: 53 with CIA and 109 matched comparators. Median follow-up time was similar between groups (CIA 3.7 vs. comparator 3.3 years, P = 0.64). There was no difference in postoperative complications, surgical revision, or death between groups. Only 32% of patients with CIA saw a rheumatologist in the outpatient setting and 33% received immunosuppressive treatment. On surveillance imaging, no difference was seen in new or worsening aortic aneurysms, but there were significantly more vascular abnormalities in branch arteries of the thoracic aorta in patients with CIA (39% vs. 11%, P < 0.01).</p><p><strong>Conclusion: </strong>Among patients who underwent surgical repair of a thoracic aortic aneurysm, patients with CIA were more likely than noninflammatory comparators to develop radiographic abnormalities in aortic branch arteries. Notably, there was no difference in risk of new aortic aneurysms or surgical complications despite most patients with CIA never receiving immunosuppression. This suggests that more selective initiation of immunosuppression in CIA may be considered after aortic aneurysm repair.</p>","PeriodicalId":7084,"journal":{"name":"ACR Open Rheumatology","volume":"4 12","pages":"1013-1020"},"PeriodicalIF":0.0000,"publicationDate":"2022-12-01","publicationTypes":"Journal Article","fieldsOfStudy":null,"isOpenAccess":false,"openAccessPdf":"https://ftp.ncbi.nlm.nih.gov/pub/pmc/oa_pdf/54/cd/ACR2-4-1013.PMC9746662.pdf","citationCount":"1","resultStr":null,"platform":"Semanticscholar","paperid":null,"PeriodicalName":"ACR Open Rheumatology","FirstCategoryId":"1085","ListUrlMain":"https://doi.org/10.1002/acr2.11504","RegionNum":0,"RegionCategory":null,"ArticlePicture":[],"TitleCN":null,"AbstractTextCN":null,"PMCID":null,"EPubDate":"","PubModel":"","JCR":"","JCRName":"","Score":null,"Total":0}
引用次数: 1
Abstract
Objective: The optimal management of patients with incidentally found clinically isolated aortitis (CIA) after aneurysm repair is unclear. This study compared long-term surgical and clinical outcomes after surgical repair of thoracic aortic aneurysm between patients with CIA and patients with noninflammatory etiologies.
Methods: This is a matched cohort study. Patients with CIA were identified by histopathology following open thoracic aortic aneurysm repair. Two comparators without inflammation on pathology were matched to each patient by year of surgical repair. Outcomes included surgical complications, new vascular abnormalities on imaging, and death.
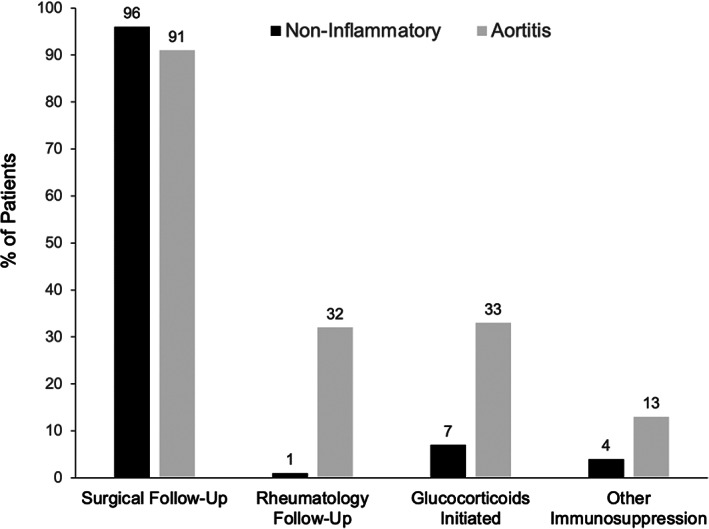
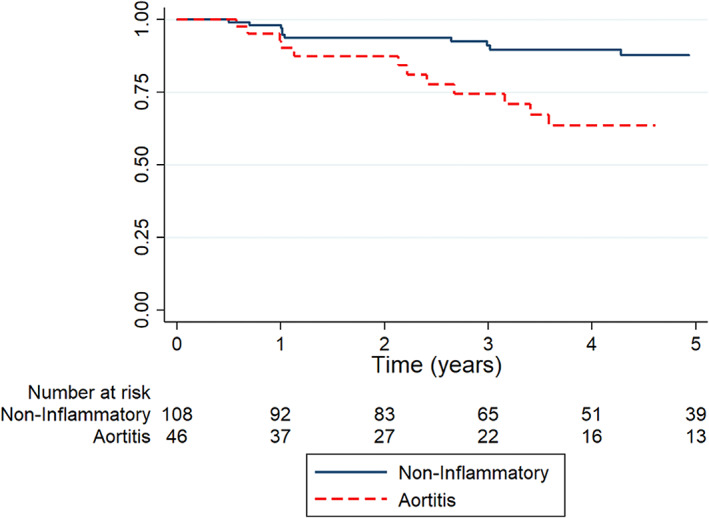
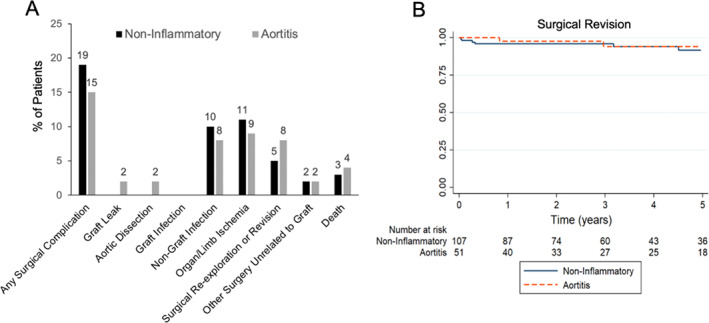
Results: One hundred sixty-two patients were included: 53 with CIA and 109 matched comparators. Median follow-up time was similar between groups (CIA 3.7 vs. comparator 3.3 years, P = 0.64). There was no difference in postoperative complications, surgical revision, or death between groups. Only 32% of patients with CIA saw a rheumatologist in the outpatient setting and 33% received immunosuppressive treatment. On surveillance imaging, no difference was seen in new or worsening aortic aneurysms, but there were significantly more vascular abnormalities in branch arteries of the thoracic aorta in patients with CIA (39% vs. 11%, P < 0.01).
Conclusion: Among patients who underwent surgical repair of a thoracic aortic aneurysm, patients with CIA were more likely than noninflammatory comparators to develop radiographic abnormalities in aortic branch arteries. Notably, there was no difference in risk of new aortic aneurysms or surgical complications despite most patients with CIA never receiving immunosuppression. This suggests that more selective initiation of immunosuppression in CIA may be considered after aortic aneurysm repair.

 求助内容:
求助内容: 应助结果提醒方式:
应助结果提醒方式:


