Exploring mutation specific beta blocker pharmacology of the pathogenic late sodium channel current from patient-specific pluripotent stem cell myocytes derived from long QT syndrome mutation carriers.
Thomas W Comollo, Xinle Zou, Chuangeng Zhang, Divya Kesters, Thomas Hof, Kevin J Sampson, Robert S Kass
{"title":"Exploring mutation specific beta blocker pharmacology of the pathogenic late sodium channel current from patient-specific pluripotent stem cell myocytes derived from long QT syndrome mutation carriers.","authors":"Thomas W Comollo, Xinle Zou, Chuangeng Zhang, Divya Kesters, Thomas Hof, Kevin J Sampson, Robert S Kass","doi":"10.1080/19336950.2022.2106025","DOIUrl":null,"url":null,"abstract":"<p><p>The congenital long QT syndrome (LQTS), one of the most common cardiac channelopathies, is characterized by delayed ventricular repolarization underlying prolongation of the QT interval of the surface electrocardiogram. LQTS is caused by mutations in genes coding for cardiac ion channels or ion channel-associated proteins. The major therapeutic approach to LQTS management is beta blocker therapy which has been shown to be effective in treatment of LQTS variants caused by mutations in K<sup>+</sup> channels. However, this approach has been questioned in the treatment of patients identified as LQTS variant 3(LQT3) patients who carry mutations in <i>SCN5A</i>, the gene coding for the principal cardiac Na<sup>+</sup> channel. LQT3 mutations are gain of function mutations that disrupt spontaneous Na<sup>+</sup> channel inactivation and promote persistent or late Na<sup>+</sup> channel current (I<sub>NaL</sub>) that delays repolarization and underlies QT prolongation. Clinical investigation of patients with the two most common LQT3 mutations, the ΔKPQ and the E1784K mutations, found beta blocker treatment a useful therapeutic approach for managing arrhythmias in this patient population. However, there is little experimental data that reveals the mechanisms underlying these antiarrhythmic actions. Here, we have investigated the effects of the beta blocker propranolol on I<sub>NaL</sub> expressed by ΔKPQ and E1784K channels in induced pluripotent stem cells derived from patients carrying these mutations. Our results indicate that propranolol preferentially inhibits I<sub>NaL</sub> expressed by these channels suggesting that the protective effects of propranolol in treating LQT3 patients is due in part to modulation of I<sub>NaL</sub>.</p>","PeriodicalId":72555,"journal":{"name":"Channels (Austin, Tex.)","volume":"16 1","pages":"173-184"},"PeriodicalIF":0.0000,"publicationDate":"2022-12-01","publicationTypes":"Journal Article","fieldsOfStudy":null,"isOpenAccess":false,"openAccessPdf":"https://www.ncbi.nlm.nih.gov/pmc/articles/PMC9373745/pdf/","citationCount":"1","resultStr":null,"platform":"Semanticscholar","paperid":null,"PeriodicalName":"Channels (Austin, Tex.)","FirstCategoryId":"1085","ListUrlMain":"https://doi.org/10.1080/19336950.2022.2106025","RegionNum":0,"RegionCategory":null,"ArticlePicture":[],"TitleCN":null,"AbstractTextCN":null,"PMCID":null,"EPubDate":"","PubModel":"","JCR":"","JCRName":"","Score":null,"Total":0}
引用次数: 1
Abstract
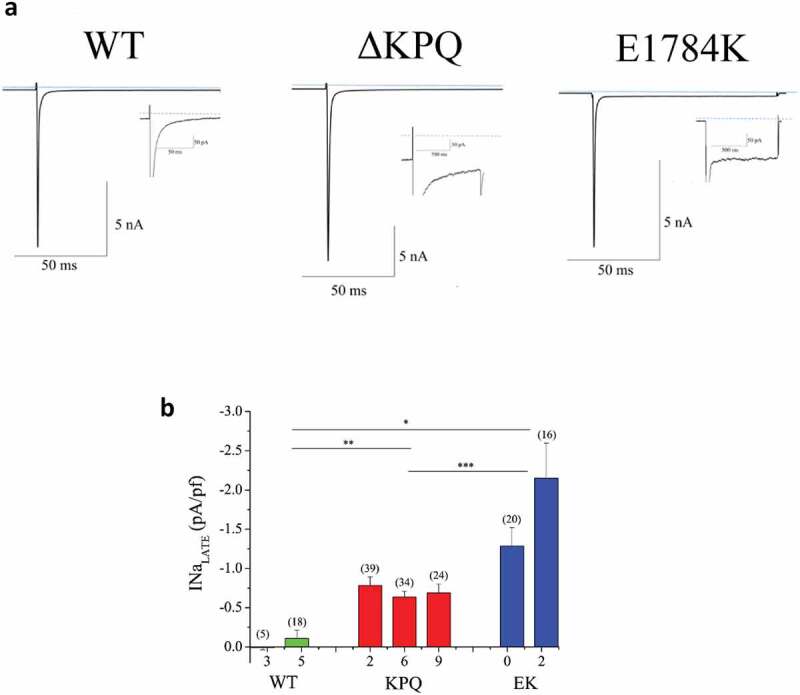
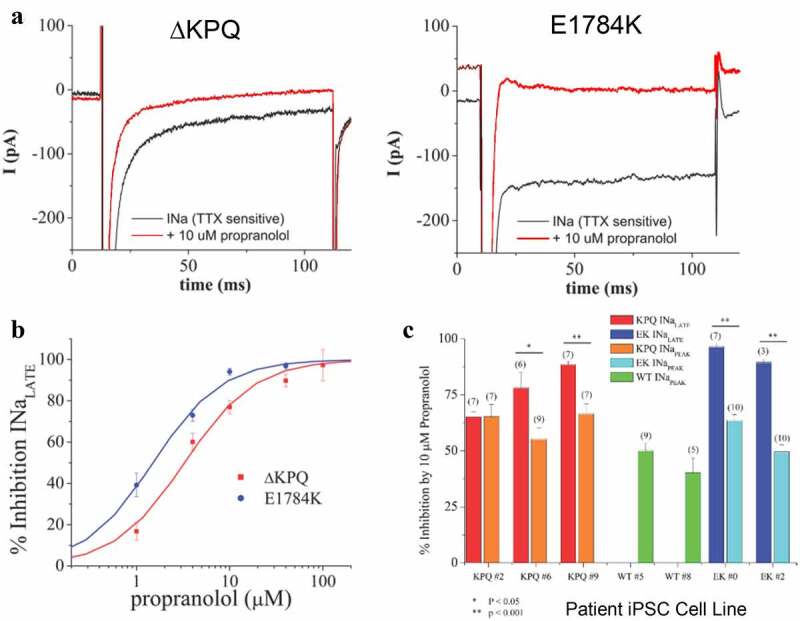
The congenital long QT syndrome (LQTS), one of the most common cardiac channelopathies, is characterized by delayed ventricular repolarization underlying prolongation of the QT interval of the surface electrocardiogram. LQTS is caused by mutations in genes coding for cardiac ion channels or ion channel-associated proteins. The major therapeutic approach to LQTS management is beta blocker therapy which has been shown to be effective in treatment of LQTS variants caused by mutations in K+ channels. However, this approach has been questioned in the treatment of patients identified as LQTS variant 3(LQT3) patients who carry mutations in SCN5A, the gene coding for the principal cardiac Na+ channel. LQT3 mutations are gain of function mutations that disrupt spontaneous Na+ channel inactivation and promote persistent or late Na+ channel current (INaL) that delays repolarization and underlies QT prolongation. Clinical investigation of patients with the two most common LQT3 mutations, the ΔKPQ and the E1784K mutations, found beta blocker treatment a useful therapeutic approach for managing arrhythmias in this patient population. However, there is little experimental data that reveals the mechanisms underlying these antiarrhythmic actions. Here, we have investigated the effects of the beta blocker propranolol on INaL expressed by ΔKPQ and E1784K channels in induced pluripotent stem cells derived from patients carrying these mutations. Our results indicate that propranolol preferentially inhibits INaL expressed by these channels suggesting that the protective effects of propranolol in treating LQT3 patients is due in part to modulation of INaL.


 求助内容:
求助内容: 应助结果提醒方式:
应助结果提醒方式:


