HEAR SCORE: A Proposal to Use Only Anamnestic and EKG Data to Evaluate Patients with Very Low Risk Chest Pain.
IF 1.5
Q3 EMERGENCY MEDICINE
引用次数: 0
Abstract
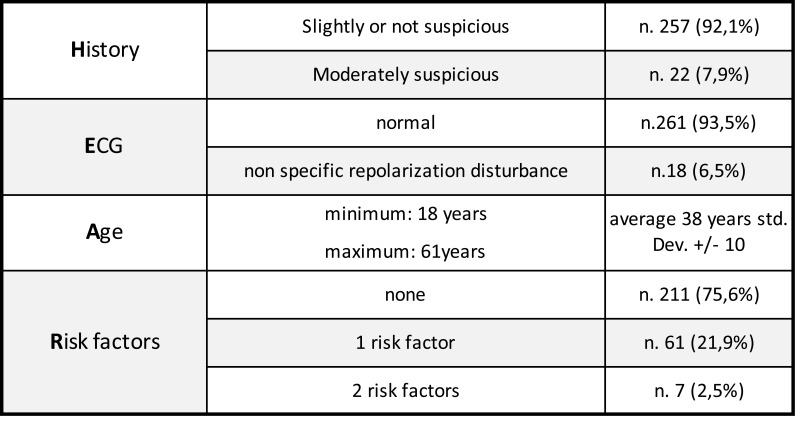
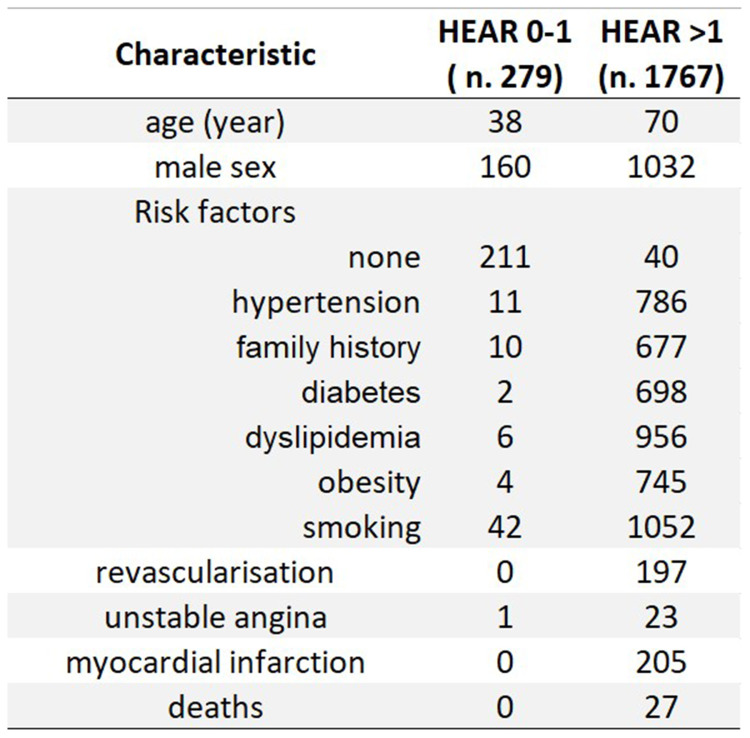
Purpose Chest pain in a common symptom in patients attending Emergency Department worldwide and can be related to an extensive variety of disorders, so it represents a diagnostic and logistic challenge for Emergency physicians. The aim of this study is to identify a subgroup of patients with a low pre-test probability of major adverse cardiac events, for which there is no need of troponin testing, to avoid potential harm from false-positive testing and long length stay in ED. Patients and Methods We retrospectively analyzed data of patients that attended ED of Siena complaining chest pain from January 2019 to August 2021. We used a modified HEART score, only evaluating history, EKG, age and risk factors. A 0–1 HEAR score was considered at very low risk for adverse cardiac events. Sensitivity, specificity, PPV, NPV and incidence of adverse cardiac events were calculated. The accuracy of HEAR score was evaluated with ROC curve. The correlation of adverse cardiac events with HEAR score 0–1 was evaluated with Fisher test. Results In this study, we included 2046 patients, of which 279 were classified at very low risk. The incidence of adverse cardiac events in this population was 0.36%. Sensibility was 97.5%, sensitivity 61%, PPV 36.8%, NPV 99.1%. The AUC for global accuracy of HEAR score was 0.945. Chi-square’s P value for the association between adverse cardiac events and HEAR score 0–1 was <0.001. Conclusion The draft presented in this study answers to the necessity to make a personalized path for patients attending ED with chest pain. The choice to avoid troponin testing may appear risky, but data from this study and from other similar show that a careful evaluation of clinical data and EKG allows to correctly discriminate which patients will not have adverse cardiac events, reducing the length of stay in ED.

听力评分:建议仅使用记忆和心电图数据来评估极低风险胸痛患者。
目的:胸痛是世界各地急诊科就诊患者的常见症状,可能与多种疾病有关,因此对急诊医生来说,胸痛是一种诊断和后勤挑战。本研究的目的是确定一个检测前主要心脏不良事件概率低的患者亚组,这些患者不需要进行肌钙蛋白检测,以避免假阳性检测和长时间住院的潜在危害。患者和方法:我们回顾性分析了2019年1月至2021年8月在锡耶纳急诊科就诊的胸痛患者的数据。我们使用改良的HEART评分,仅评估病史、心电图、年龄和危险因素。0-1的听力评分被认为是心脏不良事件的极低风险。计算敏感性、特异性、PPV、NPV和心脏不良事件发生率。采用ROC曲线评价听力评分的准确性。采用Fisher检验评价心脏不良事件与HEAR评分0-1的相关性。结果:本研究纳入2046例患者,其中279例为极低风险。该人群心脏不良事件发生率为0.36%。敏感性97.5%,敏感性61%,PPV 36.8%, NPV 99.1%。听力评分整体准确度的AUC为0.945。心脏不良事件与HEAR评分0-1之间相关性的卡方P值为:结论:本研究提出的草案回答了为胸痛急诊科患者制定个性化路径的必要性。避免肌钙蛋白检测的选择可能看起来有风险,但本研究和其他类似研究的数据表明,仔细评估临床数据和心电图可以正确区分哪些患者不会发生不良心脏事件,从而减少在急诊科的住院时间。
本文章由计算机程序翻译,如有差异,请以英文原文为准。
求助全文
约1分钟内获得全文
求助全文
来源期刊

Open Access Emergency Medicine
EMERGENCY MEDICINE-
CiteScore
2.60
自引率
6.70%
发文量
85
审稿时长
16 weeks
文献相关原料
| 公司名称 | 产品信息 | 采购帮参考价格 |
|---|
 求助内容:
求助内容: 应助结果提醒方式:
应助结果提醒方式:


