{"title":"Severe bloody diarrhea due to cytokine release syndrome after chimeric antigen receptor T cell therapy for refractory acute lymphoblastic leukemia.","authors":"Haruko Shima, Takahiro Ishikawa, Jumpei Ito, Katsura Emoto, Takumi Kurosawa, Dai Keino, Fumito Yamazaki, Hiroaki Goto, Hiroyuki Shimada","doi":"10.31547/bct-2021-009","DOIUrl":null,"url":null,"abstract":"<p><p>Cytokine release syndrome (CRS), which may be associated with fever, hypotension, hypoxia, and organ damage, is caused by a massive cytokine release after chimeric antigen receptor (CAR)-T cell therapy. We present the case of a patient who developed severe bloody diarrhea due to CRS after CAR-T cell infusion. A 10-year-old boy presented with a second relapse of B-cell precursor acute lymphoblastic leukemia 6 months after hematopoietic stem cell transplantation from an unrelated donor. CAR-T cells (tisagenlecleucel) were infused at the third complete remission after salvage chemotherapy. While fever >39°C was sustained from day 4, circulatory and respiratory status remained stable. However, he experienced severe bloody diarrhea. There was no evidence of infection; lower gastrointestinal (GI) endoscopy revealed extensive edema with erosion and ulceration, suggestive of non-specific intestinal inflammation. Thus, we considered CRS-associated grade 3 GI damage and administered a single dose of tocilizumab for grade 2 CRS, followed by 4 days of corticosteroids. Afterwards, no fever or GI bleeding was observed. Biopsy of the intestinal mucosa revealed ulcerative change with a lack of epithelial cells, which may correspond to histologic grade 4 graft versus host disease (GVHD). However, diarrhea corresponded to stage 1 GVHD, and the GVHD risk after CAR-T cell infusion has been reported to be rare in clinical practice. Although severe GI symptoms associated with CRS after CAR-T therapy are rare, early tocilizumab use is recommended for non-infectious severe GI symptoms to avoid long-term corticosteroid use, which may reduce CAR-T cell efficacy.</p>","PeriodicalId":72423,"journal":{"name":"Blood cell therapy","volume":"5 1","pages":"31-34"},"PeriodicalIF":0.0000,"publicationDate":"2022-02-25","publicationTypes":"Journal Article","fieldsOfStudy":null,"isOpenAccess":false,"openAccessPdf":"https://ftp.ncbi.nlm.nih.gov/pub/pmc/oa_pdf/ae/f5/2432-7026-5-1-0031.PMC9847265.pdf","citationCount":"0","resultStr":null,"platform":"Semanticscholar","paperid":null,"PeriodicalName":"Blood cell therapy","FirstCategoryId":"1085","ListUrlMain":"https://doi.org/10.31547/bct-2021-009","RegionNum":0,"RegionCategory":null,"ArticlePicture":[],"TitleCN":null,"AbstractTextCN":null,"PMCID":null,"EPubDate":"","PubModel":"","JCR":"","JCRName":"","Score":null,"Total":0}
引用次数: 0
Abstract
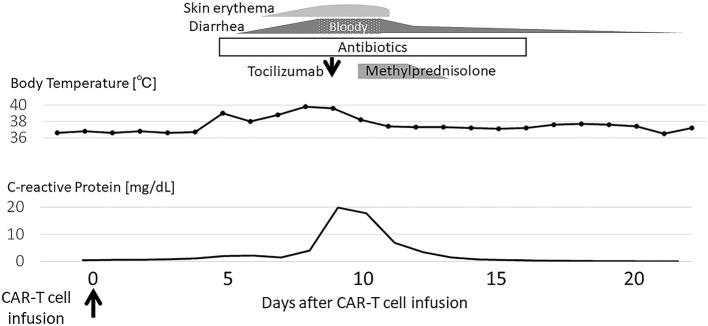
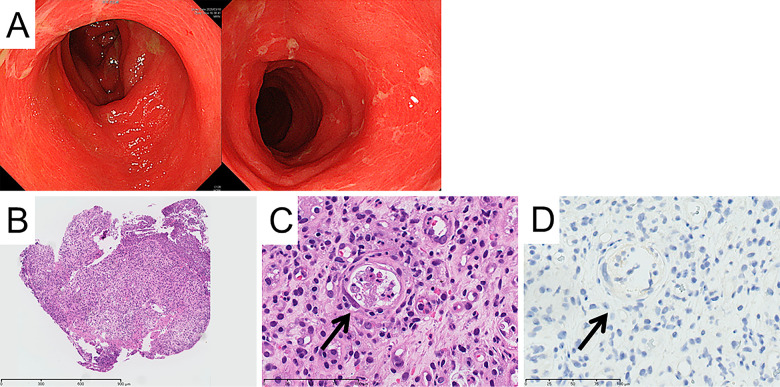
Cytokine release syndrome (CRS), which may be associated with fever, hypotension, hypoxia, and organ damage, is caused by a massive cytokine release after chimeric antigen receptor (CAR)-T cell therapy. We present the case of a patient who developed severe bloody diarrhea due to CRS after CAR-T cell infusion. A 10-year-old boy presented with a second relapse of B-cell precursor acute lymphoblastic leukemia 6 months after hematopoietic stem cell transplantation from an unrelated donor. CAR-T cells (tisagenlecleucel) were infused at the third complete remission after salvage chemotherapy. While fever >39°C was sustained from day 4, circulatory and respiratory status remained stable. However, he experienced severe bloody diarrhea. There was no evidence of infection; lower gastrointestinal (GI) endoscopy revealed extensive edema with erosion and ulceration, suggestive of non-specific intestinal inflammation. Thus, we considered CRS-associated grade 3 GI damage and administered a single dose of tocilizumab for grade 2 CRS, followed by 4 days of corticosteroids. Afterwards, no fever or GI bleeding was observed. Biopsy of the intestinal mucosa revealed ulcerative change with a lack of epithelial cells, which may correspond to histologic grade 4 graft versus host disease (GVHD). However, diarrhea corresponded to stage 1 GVHD, and the GVHD risk after CAR-T cell infusion has been reported to be rare in clinical practice. Although severe GI symptoms associated with CRS after CAR-T therapy are rare, early tocilizumab use is recommended for non-infectious severe GI symptoms to avoid long-term corticosteroid use, which may reduce CAR-T cell efficacy.

 求助内容:
求助内容: 应助结果提醒方式:
应助结果提醒方式:


