Maulik K Lathiya, Praveen Errabelli, Susan M Cullinan, Emeka J Amadi
{"title":"Severe hypernatremia in hyperglycemic conditions; managing it effectively: A case report.","authors":"Maulik K Lathiya, Praveen Errabelli, Susan M Cullinan, Emeka J Amadi","doi":"10.5492/wjccm.v12.i1.29","DOIUrl":null,"url":null,"abstract":"<p><strong>Background: </strong>Diabetic ketoacidosis (DKA) and hyperglycemic hyperosmolar state (HHS) are common acute complications of diabetes mellitus with a high risk of mortality. When combined with hypernatremia, the complications can be even worse. Hypernatremia is a rarely associated with DKA and HHS as both are usually accompanied by normal sodium or hyponatremia. As a result, a structured and systematic treatment approach is critical. We discuss the therapeutic approach and implications of this uncommon presentation.</p><p><strong>Case summary: </strong>A 62-year-old man with no known past medical history presented to emergency department with altered mental status. Initial work up in emergency room showed severe hyperglycemia with a glucose level of 1093 mg/dL and severe hypernatremia with a serum sodium level of 169 mEq/L. He was admitted to the intensive care unit (ICU) and was started on insulin drip as <i>per</i> DKA protocol. Within 12 h of ICU admission, blood sugar was 300 mg/dL. But his mental status didn't show much improvement. He was dehydrated and had a corrected serum sodium level of > 190 mEq/L. As a result, dextrose 5% in water and ringer's lactate were started. He was also given free water <i>via</i> an nasogastric (NG) tube and IV Desmopressin to improve his free water deficit, which improved his serum sodium to 140 mEq/L.</p><p><strong>Conclusion: </strong>The combination of DKA, HHS and hypernatremia is rare and extremely challenging to manage, but the most challenging part of this condition is selecting the correct type of fluids to treat these conditions. Our case illustrates that desmopressin and free water administration <i>via</i> the NG route can be helpful in this situation.</p>","PeriodicalId":66959,"journal":{"name":"世界危重病急救学杂志(英文版)","volume":"12 1","pages":"29-34"},"PeriodicalIF":0.0000,"publicationDate":"2023-01-09","publicationTypes":"Journal Article","fieldsOfStudy":null,"isOpenAccess":false,"openAccessPdf":"https://ftp.ncbi.nlm.nih.gov/pub/pmc/oa_pdf/b4/8e/WJCCM-12-29.PMC9846872.pdf","citationCount":"0","resultStr":null,"platform":"Semanticscholar","paperid":null,"PeriodicalName":"世界危重病急救学杂志(英文版)","FirstCategoryId":"1085","ListUrlMain":"https://doi.org/10.5492/wjccm.v12.i1.29","RegionNum":0,"RegionCategory":null,"ArticlePicture":[],"TitleCN":null,"AbstractTextCN":null,"PMCID":null,"EPubDate":"","PubModel":"","JCR":"","JCRName":"","Score":null,"Total":0}
引用次数: 0
Abstract
Background: Diabetic ketoacidosis (DKA) and hyperglycemic hyperosmolar state (HHS) are common acute complications of diabetes mellitus with a high risk of mortality. When combined with hypernatremia, the complications can be even worse. Hypernatremia is a rarely associated with DKA and HHS as both are usually accompanied by normal sodium or hyponatremia. As a result, a structured and systematic treatment approach is critical. We discuss the therapeutic approach and implications of this uncommon presentation.
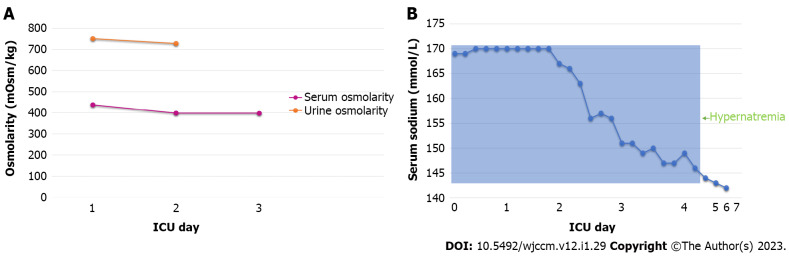
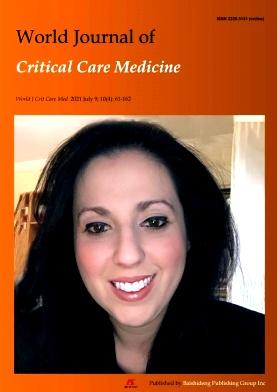
Case summary: A 62-year-old man with no known past medical history presented to emergency department with altered mental status. Initial work up in emergency room showed severe hyperglycemia with a glucose level of 1093 mg/dL and severe hypernatremia with a serum sodium level of 169 mEq/L. He was admitted to the intensive care unit (ICU) and was started on insulin drip as per DKA protocol. Within 12 h of ICU admission, blood sugar was 300 mg/dL. But his mental status didn't show much improvement. He was dehydrated and had a corrected serum sodium level of > 190 mEq/L. As a result, dextrose 5% in water and ringer's lactate were started. He was also given free water via an nasogastric (NG) tube and IV Desmopressin to improve his free water deficit, which improved his serum sodium to 140 mEq/L.
Conclusion: The combination of DKA, HHS and hypernatremia is rare and extremely challenging to manage, but the most challenging part of this condition is selecting the correct type of fluids to treat these conditions. Our case illustrates that desmopressin and free water administration via the NG route can be helpful in this situation.
 求助内容:
求助内容: 应助结果提醒方式:
应助结果提醒方式:


