Nazima Khatun, Yonatan Akivis, Beisi Ji, Harshith P Chandrakumar, Inna Bukharovich, Sabu John
{"title":"Tuberculous Pericarditis Presenting as Cardiac Tamponade: Role of Echocardiography.","authors":"Nazima Khatun, Yonatan Akivis, Beisi Ji, Harshith P Chandrakumar, Inna Bukharovich, Sabu John","doi":"10.14740/jmc4119","DOIUrl":null,"url":null,"abstract":"<p><p>Tuberculous pericarditis, a rare but potentially lethal manifestation of tuberculosis, poses diagnostic and therapeutic challenges in clinical practice. Its nonspecific clinical presentation often mimics other conditions, leading to delayed or missed diagnoses. We report a 25-year-old male with no past medical history, who presented with nonspecific symptoms such as fatigue, weight loss, body aches, and dyspnea. An electrocardiogram showed low voltage QRS complex with electrical alternans, and transthoracic echocardiography (TTE) showed large pericardial effusion with tamponade physiology with right ventricular diastolic collapse, the collapse of the right atrium and the inferior vena cava was dilated with a respiratory variation of less than 50%. The diagnosis of tuberculous pericarditis was made based on clinical presentation, imaging, and laboratory findings, including a positive QuantiFERON-TB gold test and pericardial fluid analysis, despite negative cultures. This case highlights the significance of considering tuberculosis in the differential diagnosis of pericardial effusion and underscores the role of imaging and laboratory investigations in diagnosis. Management of tuberculous pericarditis involves a combination of antituberculous chemotherapy, pericardiocentesis, and corticosteroids. Despite its rarity, tuberculous pericarditis carries a high mortality rate and can present as cardiac tamponade, as illustrated in our case. This underscores the need for high clinical suspicion, especially in high-risk populations, for timely diagnosis and initiation of treatment.</p>","PeriodicalId":16279,"journal":{"name":"Journal of Medical Cases","volume":"14 8","pages":"271-276"},"PeriodicalIF":0.0000,"publicationDate":"2023-08-01","publicationTypes":"Journal Article","fieldsOfStudy":null,"isOpenAccess":false,"openAccessPdf":"https://ftp.ncbi.nlm.nih.gov/pub/pmc/oa_pdf/43/8d/jmc-14-271.PMC10482598.pdf","citationCount":"0","resultStr":null,"platform":"Semanticscholar","paperid":null,"PeriodicalName":"Journal of Medical Cases","FirstCategoryId":"1085","ListUrlMain":"https://doi.org/10.14740/jmc4119","RegionNum":0,"RegionCategory":null,"ArticlePicture":[],"TitleCN":null,"AbstractTextCN":null,"PMCID":null,"EPubDate":"","PubModel":"","JCR":"","JCRName":"","Score":null,"Total":0}
引用次数: 0
Abstract
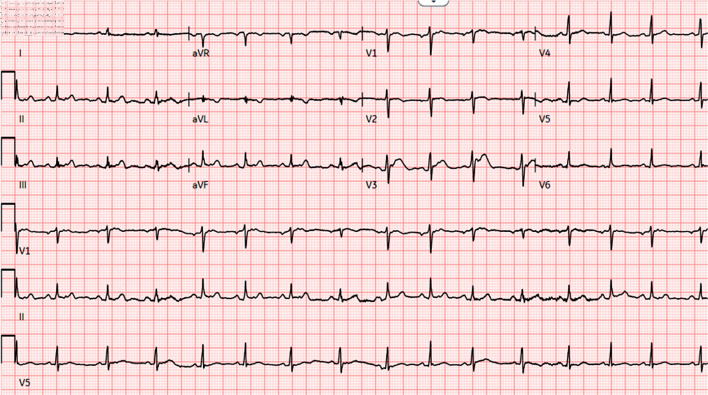
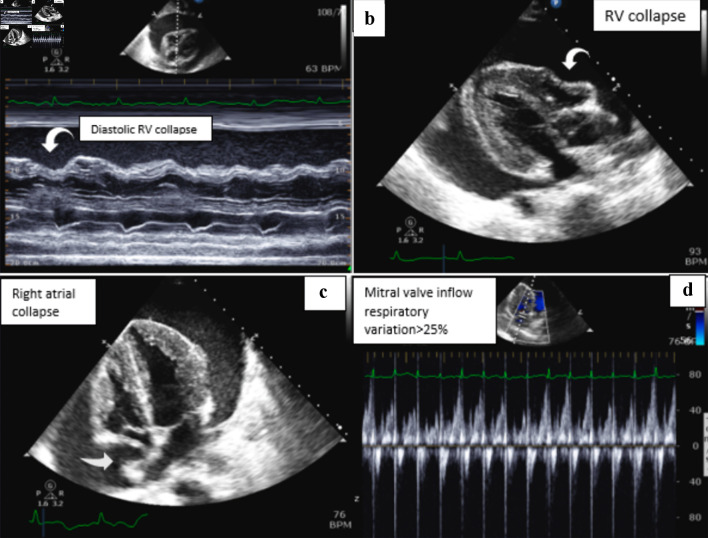
Tuberculous pericarditis, a rare but potentially lethal manifestation of tuberculosis, poses diagnostic and therapeutic challenges in clinical practice. Its nonspecific clinical presentation often mimics other conditions, leading to delayed or missed diagnoses. We report a 25-year-old male with no past medical history, who presented with nonspecific symptoms such as fatigue, weight loss, body aches, and dyspnea. An electrocardiogram showed low voltage QRS complex with electrical alternans, and transthoracic echocardiography (TTE) showed large pericardial effusion with tamponade physiology with right ventricular diastolic collapse, the collapse of the right atrium and the inferior vena cava was dilated with a respiratory variation of less than 50%. The diagnosis of tuberculous pericarditis was made based on clinical presentation, imaging, and laboratory findings, including a positive QuantiFERON-TB gold test and pericardial fluid analysis, despite negative cultures. This case highlights the significance of considering tuberculosis in the differential diagnosis of pericardial effusion and underscores the role of imaging and laboratory investigations in diagnosis. Management of tuberculous pericarditis involves a combination of antituberculous chemotherapy, pericardiocentesis, and corticosteroids. Despite its rarity, tuberculous pericarditis carries a high mortality rate and can present as cardiac tamponade, as illustrated in our case. This underscores the need for high clinical suspicion, especially in high-risk populations, for timely diagnosis and initiation of treatment.

 求助内容:
求助内容: 应助结果提醒方式:
应助结果提醒方式:


