Alícia Molina Andújar, Victor Joaquin Escudero, Gaston J Piñeiro, Alvaro Lucas, Irene Rovira, Purificación Matute, Cristina Ibañez, Miquel Blasco, Luis F Quintana, Elena Sandoval, Marina Chorda Sánchez, Eduard Quintana, Esteban Poch
{"title":"Impact of cardiac surgery associated acute kidney injury on 1-year major adverse kidney events.","authors":"Alícia Molina Andújar, Victor Joaquin Escudero, Gaston J Piñeiro, Alvaro Lucas, Irene Rovira, Purificación Matute, Cristina Ibañez, Miquel Blasco, Luis F Quintana, Elena Sandoval, Marina Chorda Sánchez, Eduard Quintana, Esteban Poch","doi":"10.3389/fneph.2023.1059668","DOIUrl":null,"url":null,"abstract":"<p><strong>Background: </strong>The incidence of acute kidney injury following cardiac surgery (CSA-AKI) is up to 30%, and the risk of chronic kidney disease (CKD) has been found to be higher in these patients compared to the AKI-free population. The aim of our study was to assess the risk of major adverse kidney events (MAKE) [25% or greater decline in estimated glomerular filtration rate (eGFR), new hemodialysis, and death] after cardiac surgery in a Spanish cohort and to evaluate the utility of the score developed by Legouis D et al. (CSA-CKD score) in predicting the occurrence of MAKE.</p><p><strong>Methods: </strong>This was a single-center retrospective study of patients who required cardiac surgery with cardiopulmonary bypass (CPB) during 2015, with a 1-year follow-up after the intervention. The inclusion criteria were patients over 18 years old who had undergone cardiac surgery [i.e., valve substitution (VS), coronary artery bypass graft (CABG), or a combination of both procedures].</p><p><strong>Results: </strong>The number of patients with CKD (eGFR < 60 mL/min) increased from 74 (18.3%) to 97 (24%) within 1 year after surgery. The median eGFR declined from 85 to 82 mL/min in the non-CSA-AKI patient group and from 73 to 65 mL/min in those with CSA-AKI (<i>p</i> = 0.024). Fifty-eight patients (1.4%) presented with MAKE at the 1-year follow-up. Multivariate logistic regression analysis showed that the only variable associated with MAKE was CSA-AKI [odds ratio (OR) 2.386 (1.31-4.35), <i>p</i> = 0.004]. The median CSA-CKD score was higher in the MAKE cohort [3 (2-4) vs. 2 (1-3), p < 0.001], but discrimination was poor, with a receiver operating characteristic curve (AUC) value of 0.682 (0.611-0.754).</p><p><strong>Conclusion: </strong>Any-stage CSA-AKI is associated with a risk of MAKE after 1 year. Further research into new measures that identify at-risk patients is needed so that appropriate patient follow-up can be carried out.</p>","PeriodicalId":73091,"journal":{"name":"Frontiers in nephrology","volume":"3 ","pages":"1059668"},"PeriodicalIF":0.0000,"publicationDate":"2023-01-01","publicationTypes":"Journal Article","fieldsOfStudy":null,"isOpenAccess":false,"openAccessPdf":"https://www.ncbi.nlm.nih.gov/pmc/articles/PMC10479748/pdf/","citationCount":"0","resultStr":null,"platform":"Semanticscholar","paperid":null,"PeriodicalName":"Frontiers in nephrology","FirstCategoryId":"1085","ListUrlMain":"https://doi.org/10.3389/fneph.2023.1059668","RegionNum":0,"RegionCategory":null,"ArticlePicture":[],"TitleCN":null,"AbstractTextCN":null,"PMCID":null,"EPubDate":"","PubModel":"","JCR":"","JCRName":"","Score":null,"Total":0}
引用次数: 0
Abstract
Background: The incidence of acute kidney injury following cardiac surgery (CSA-AKI) is up to 30%, and the risk of chronic kidney disease (CKD) has been found to be higher in these patients compared to the AKI-free population. The aim of our study was to assess the risk of major adverse kidney events (MAKE) [25% or greater decline in estimated glomerular filtration rate (eGFR), new hemodialysis, and death] after cardiac surgery in a Spanish cohort and to evaluate the utility of the score developed by Legouis D et al. (CSA-CKD score) in predicting the occurrence of MAKE.
Methods: This was a single-center retrospective study of patients who required cardiac surgery with cardiopulmonary bypass (CPB) during 2015, with a 1-year follow-up after the intervention. The inclusion criteria were patients over 18 years old who had undergone cardiac surgery [i.e., valve substitution (VS), coronary artery bypass graft (CABG), or a combination of both procedures].
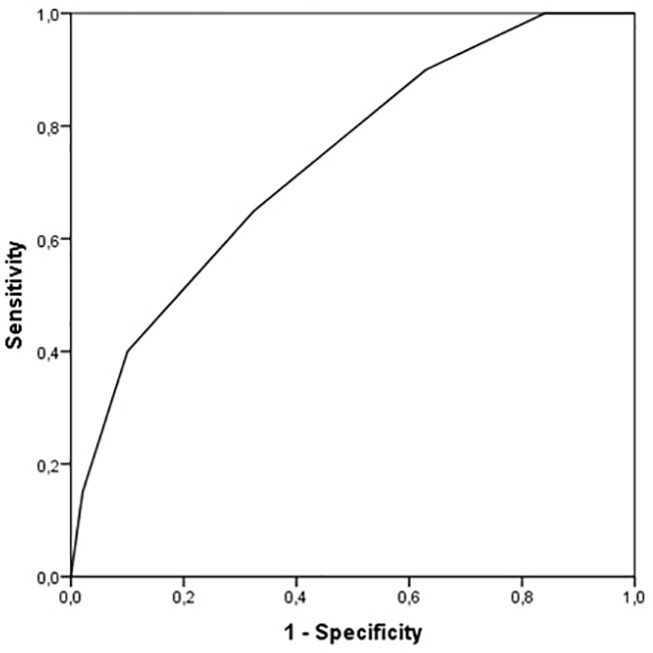
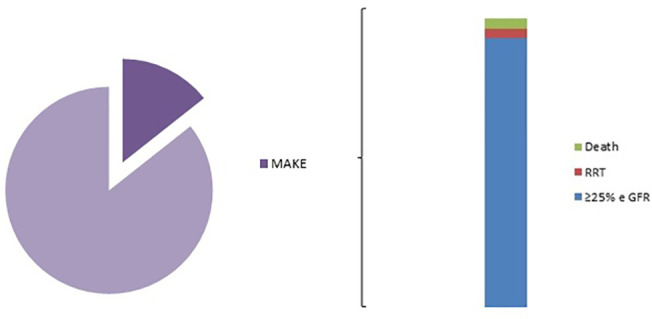
Results: The number of patients with CKD (eGFR < 60 mL/min) increased from 74 (18.3%) to 97 (24%) within 1 year after surgery. The median eGFR declined from 85 to 82 mL/min in the non-CSA-AKI patient group and from 73 to 65 mL/min in those with CSA-AKI (p = 0.024). Fifty-eight patients (1.4%) presented with MAKE at the 1-year follow-up. Multivariate logistic regression analysis showed that the only variable associated with MAKE was CSA-AKI [odds ratio (OR) 2.386 (1.31-4.35), p = 0.004]. The median CSA-CKD score was higher in the MAKE cohort [3 (2-4) vs. 2 (1-3), p < 0.001], but discrimination was poor, with a receiver operating characteristic curve (AUC) value of 0.682 (0.611-0.754).
Conclusion: Any-stage CSA-AKI is associated with a risk of MAKE after 1 year. Further research into new measures that identify at-risk patients is needed so that appropriate patient follow-up can be carried out.


 求助内容:
求助内容: 应助结果提醒方式:
应助结果提醒方式:


