D. Delport , R. Sacks-Davis , R.G. Abeysuriya , M. Hellard , N. Scott
{"title":"Lives saved by public health restrictions over the Victorian COVID-19 Delta variant epidemic wave, Aug-Nov 2021","authors":"D. Delport , R. Sacks-Davis , R.G. Abeysuriya , M. Hellard , N. Scott","doi":"10.1016/j.epidem.2023.100702","DOIUrl":null,"url":null,"abstract":"<div><h3>Background</h3><p>Prior to mid-2021, Australia’s approach to COVID-19 was to eliminate community transmission. However, between August-November 2021, the state of Victoria, Australia, experienced an outbreak of the Delta variant that continued to grow despite extensive lockdowns and public health measures in place. While these public health restrictions were ultimately unable to stop community transmission, they likely had a major impact reducing transmission and adverse health outcomes relative to voluntary risk-mitigation only (e.g., in response to rising cases and deaths, some people may avoid crowded settings, hospitality, retail, social occasions, or indoor settings). This study aims to estimate the impact of the August-November 2021 enforced public health restrictions in Victoria, compared to voluntary risk-mitigation only.</p></div><div><h3>Methods</h3><p>An agent-based model was calibrated to Victorian epidemiological, health and behavioural data from 1 August to 30 November 2021, as well as policies that were implemented over that period. Two counter-factual scenarios were run for the same period with (a) no restrictions in place; or (b) voluntary risk-mitigation only, based on behaviour measured over the December-January Omicron BA.1 epidemic wave when restrictions were not in place.</p></div><div><h3>Results</h3><p>Over August-November 2021, the baseline model scenario resulted in 97,000 (91,000−102,000) diagnoses, 9100 (8500−9700) hospital admissions, and 480 (430−530) deaths. Without any restrictions in place, there were 3,228,000 (3,200,000−3,253,000) diagnoses, 375,100 (370,200−380,900) hospital admissions, and 16,700 (16,000−17,500) deaths. With voluntary risk-mitigation equal to those observed during the Omicron BA.1 epidemic wave, there were 1,507,000 (1,469,000−1,549,000) diagnoses, 130,300 (124,500−136,000) hospital admissions, and 5500 (5000−6100) deaths.</p></div><div><h3>Conclusion</h3><p>Public health restrictions implemented in Victoria over August-November 2021 are likely to have averted more than 120,000 hospitalizations and 5000 deaths relative to voluntary risk-mitigation only. During a COVID-19 epidemic wave voluntary behaviour change can reduce transmission substantially, but not to the same extent as enforced restrictions.</p></div>","PeriodicalId":49206,"journal":{"name":"Epidemics","volume":"44 ","pages":"Article 100702"},"PeriodicalIF":3.0000,"publicationDate":"2023-09-01","publicationTypes":"Journal Article","fieldsOfStudy":null,"isOpenAccess":false,"openAccessPdf":"https://www.ncbi.nlm.nih.gov/pmc/articles/PMC10265399/pdf/","citationCount":"0","resultStr":null,"platform":"Semanticscholar","paperid":null,"PeriodicalName":"Epidemics","FirstCategoryId":"3","ListUrlMain":"https://www.sciencedirect.com/science/article/pii/S1755436523000385","RegionNum":3,"RegionCategory":"医学","ArticlePicture":[],"TitleCN":null,"AbstractTextCN":null,"PMCID":null,"EPubDate":"","PubModel":"","JCR":"Q2","JCRName":"INFECTIOUS DISEASES","Score":null,"Total":0}
引用次数: 0
Abstract
Background
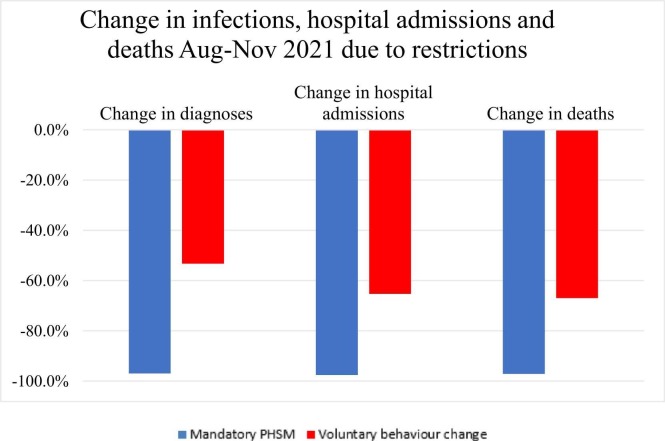
Prior to mid-2021, Australia’s approach to COVID-19 was to eliminate community transmission. However, between August-November 2021, the state of Victoria, Australia, experienced an outbreak of the Delta variant that continued to grow despite extensive lockdowns and public health measures in place. While these public health restrictions were ultimately unable to stop community transmission, they likely had a major impact reducing transmission and adverse health outcomes relative to voluntary risk-mitigation only (e.g., in response to rising cases and deaths, some people may avoid crowded settings, hospitality, retail, social occasions, or indoor settings). This study aims to estimate the impact of the August-November 2021 enforced public health restrictions in Victoria, compared to voluntary risk-mitigation only.
Methods
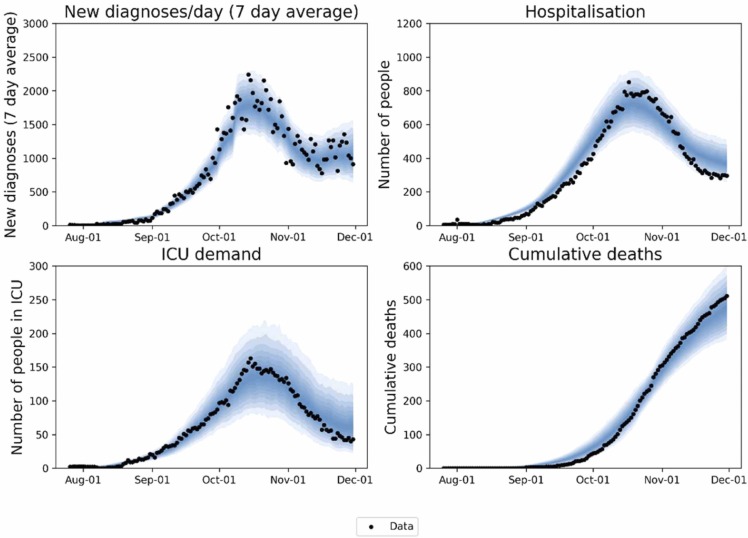
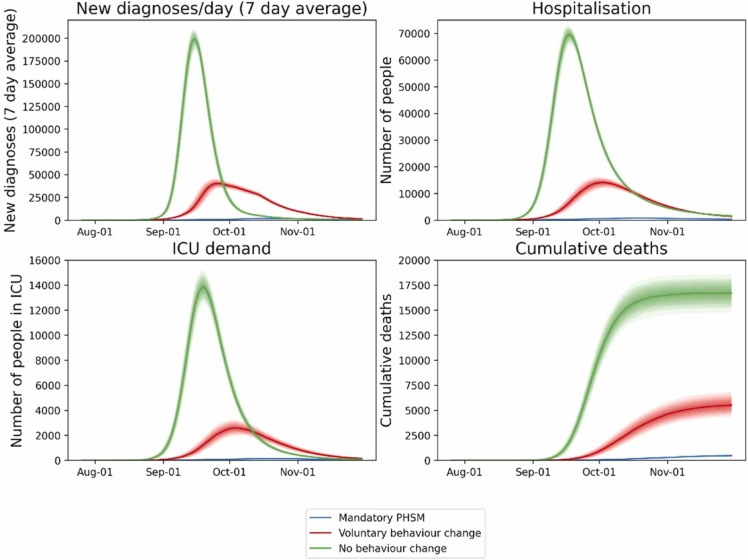
An agent-based model was calibrated to Victorian epidemiological, health and behavioural data from 1 August to 30 November 2021, as well as policies that were implemented over that period. Two counter-factual scenarios were run for the same period with (a) no restrictions in place; or (b) voluntary risk-mitigation only, based on behaviour measured over the December-January Omicron BA.1 epidemic wave when restrictions were not in place.
Results
Over August-November 2021, the baseline model scenario resulted in 97,000 (91,000−102,000) diagnoses, 9100 (8500−9700) hospital admissions, and 480 (430−530) deaths. Without any restrictions in place, there were 3,228,000 (3,200,000−3,253,000) diagnoses, 375,100 (370,200−380,900) hospital admissions, and 16,700 (16,000−17,500) deaths. With voluntary risk-mitigation equal to those observed during the Omicron BA.1 epidemic wave, there were 1,507,000 (1,469,000−1,549,000) diagnoses, 130,300 (124,500−136,000) hospital admissions, and 5500 (5000−6100) deaths.
Conclusion
Public health restrictions implemented in Victoria over August-November 2021 are likely to have averted more than 120,000 hospitalizations and 5000 deaths relative to voluntary risk-mitigation only. During a COVID-19 epidemic wave voluntary behaviour change can reduce transmission substantially, but not to the same extent as enforced restrictions.
期刊介绍:
Epidemics publishes papers on infectious disease dynamics in the broadest sense. Its scope covers both within-host dynamics of infectious agents and dynamics at the population level, particularly the interaction between the two. Areas of emphasis include: spread, transmission, persistence, implications and population dynamics of infectious diseases; population and public health as well as policy aspects of control and prevention; dynamics at the individual level; interaction with the environment, ecology and evolution of infectious diseases, as well as population genetics of infectious agents.

 求助内容:
求助内容: 应助结果提醒方式:
应助结果提醒方式:


