{"title":"Comparison of antipsychotic prescribing practices following failure of antipsychotic monotherapy in the acute care setting.","authors":"Kaitlyn Morgan, Leah Rickert","doi":"10.9740/mhc.2022.12.329","DOIUrl":null,"url":null,"abstract":"<p><strong>Introduction: </strong>Numerous strategies exist following antipsychotic monotherapy failure including transition to another antipsychotic, dosing above FDA recommendations, or dual antipsychotic therapy. This study described antipsychotic prescribing practices on an acute psychiatry unit following antipsychotic monotherapy failure and compared outcomes to determine if any strategy resulted in superior short-term outcomes.</p><p><strong>Methods: </strong>This retrospective chart review assessed postintervention time to discharge for patients with schizophrenia or schizoaffective disorder requiring therapy change following treatment failure. Secondary outcomes included 30-day readmission rate, length of stay, and discharge chlorpromazine equivalents.</p><p><strong>Results: </strong>There were no differences in number of past antipsychotic trials between groups (4.8 vs 4.5; <i>P</i> = .73). Of all the patients, 73% (n = 30) discharged on alternative antipsychotic monotherapy while 27% (n = 11) discharged on dual antipsychotic therapy. No patients had doses increased above FDA recommendations. The alternative antipsychotic group had shorter mean postintervention time to discharge (8.8 vs 20.6 days; <i>P</i> = .003) and shorter mean length of stay (16.7 vs 32.1 days; <i>P</i> = .03). Median time to discharge was not statistically significant (6.4 vs 14.0 days; <i>P</i> = .17). The dual antipsychotic group had higher mean chlorpromazine equivalents (723 mg vs 356 mg; <i>P</i> = .002). There was no difference in 30-day readmission rates (16.7% vs 27.3%; χ<sup>2</sup> = 0.5765; <i>P</i> = .45).</p><p><strong>Discussion: </strong>This study found that following failure of antipsychotic monotherapy, transition to an alternative antipsychotic was associated with decreased mean time to discharge as compared to dual antipsychotic therapy. Further studies are needed to assess long-term clinical implications of these findings.</p>","PeriodicalId":22710,"journal":{"name":"The Mental Health Clinician","volume":"12 6","pages":"329-335"},"PeriodicalIF":0.0000,"publicationDate":"2023-01-05","publicationTypes":"Journal Article","fieldsOfStudy":null,"isOpenAccess":false,"openAccessPdf":"https://ftp.ncbi.nlm.nih.gov/pub/pmc/oa_pdf/3c/a9/i2168-9709-12-6-329.PMC9819140.pdf","citationCount":"0","resultStr":null,"platform":"Semanticscholar","paperid":null,"PeriodicalName":"The Mental Health Clinician","FirstCategoryId":"1085","ListUrlMain":"https://doi.org/10.9740/mhc.2022.12.329","RegionNum":0,"RegionCategory":null,"ArticlePicture":[],"TitleCN":null,"AbstractTextCN":null,"PMCID":null,"EPubDate":"2022/12/1 0:00:00","PubModel":"eCollection","JCR":"","JCRName":"","Score":null,"Total":0}
引用次数: 0
Abstract
Introduction: Numerous strategies exist following antipsychotic monotherapy failure including transition to another antipsychotic, dosing above FDA recommendations, or dual antipsychotic therapy. This study described antipsychotic prescribing practices on an acute psychiatry unit following antipsychotic monotherapy failure and compared outcomes to determine if any strategy resulted in superior short-term outcomes.
Methods: This retrospective chart review assessed postintervention time to discharge for patients with schizophrenia or schizoaffective disorder requiring therapy change following treatment failure. Secondary outcomes included 30-day readmission rate, length of stay, and discharge chlorpromazine equivalents.
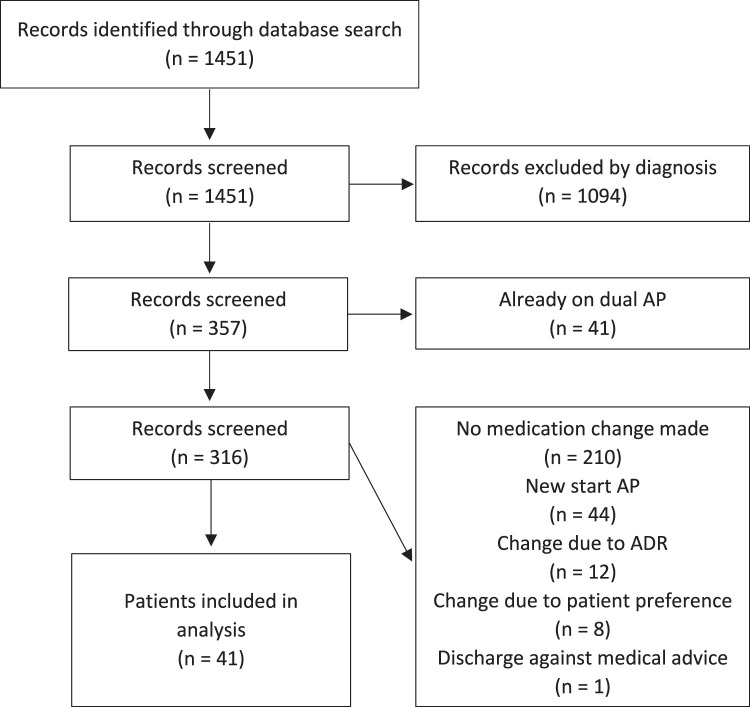
Results: There were no differences in number of past antipsychotic trials between groups (4.8 vs 4.5; P = .73). Of all the patients, 73% (n = 30) discharged on alternative antipsychotic monotherapy while 27% (n = 11) discharged on dual antipsychotic therapy. No patients had doses increased above FDA recommendations. The alternative antipsychotic group had shorter mean postintervention time to discharge (8.8 vs 20.6 days; P = .003) and shorter mean length of stay (16.7 vs 32.1 days; P = .03). Median time to discharge was not statistically significant (6.4 vs 14.0 days; P = .17). The dual antipsychotic group had higher mean chlorpromazine equivalents (723 mg vs 356 mg; P = .002). There was no difference in 30-day readmission rates (16.7% vs 27.3%; χ2 = 0.5765; P = .45).
Discussion: This study found that following failure of antipsychotic monotherapy, transition to an alternative antipsychotic was associated with decreased mean time to discharge as compared to dual antipsychotic therapy. Further studies are needed to assess long-term clinical implications of these findings.

 求助内容:
求助内容: 应助结果提醒方式:
应助结果提醒方式:


