Manisha Verma, Radi Zaki, Johnathan Sadeh, John P Knorr, Mark Gallagher, Afshin Parsikia, Victor Navarro
{"title":"Improved Medication Adherence with the Use of Extended-Release Tacrolimus in Liver Transplant Recipients: A Pilot Randomized Controlled Trial.","authors":"Manisha Verma, Radi Zaki, Johnathan Sadeh, John P Knorr, Mark Gallagher, Afshin Parsikia, Victor Navarro","doi":"10.1155/2023/7915781","DOIUrl":null,"url":null,"abstract":"<p><strong>Background: </strong>Nonadherence to immunosuppression in liver transplant recipients (LTRs) leads to deterioration in health outcomes. Once-dailyextended-release tacrolimus (TAC-ER) may improve adherence when compared to twice-dailyimmediate-release tacrolimus (TAC-IR).</p><p><strong>Methods: </strong>We conducted a randomized controlled study to evaluate medication adherence, clinical efficacy, and safety of TAC-ER in stable LTR. All patients >18 years who underwent liver transplantation before 6 months were eligible. Patients were randomized 1 : 1 to continued TAC-IR or conversion to TAC-ER. The primary outcome was change in medication adherence from baseline to 9 months, assessed using BAASIS. Secondary outcomes were tacrolimus trough levels, safety, and quality of life.</p><p><strong>Results: </strong>Thirty-one patients were consented and randomized to either of the two groups: conversion to TAC-ER (<i>n</i> = 15) or continued TAC-IR (<i>n</i> = 16). Six patients in the TAC-ER group withdrew after randomization due to apprehension about switching medication (<i>n</i> = 2), unwillingness to travel (<i>n</i> = 2), and increased liver tests after conversion (<i>n</i> = 2, both were acute rejections despite therapeutic tacrolimus levels and were considered unrelated to TAC-ER). We compared the results of nine patients in the TAC-ER group that completed the study with those of sixteen in the TAC-IR group. At baseline, there was no difference in tacrolimus trough levels between groups. Improved adherence was observed in the TAC-ER group as 100% of patients reported at least one period of full adherence during the study period (100% vs. 62.6%, <i>p</i> = 0.035). Tacrolimus trough levels and liver tests were comparable between groups throughout the study. There were no differences in eGFR, HbA1c, or QoL between the groups.</p><p><strong>Conclusion: </strong>TAC-ER improved medication adherence while maintaining comparable trough levels, liver function, and QoL as TAC-IR in LTR.</p>","PeriodicalId":45795,"journal":{"name":"Journal of Transplantation","volume":"2023 ","pages":"7915781"},"PeriodicalIF":2.2000,"publicationDate":"2023-01-01","publicationTypes":"Journal Article","fieldsOfStudy":null,"isOpenAccess":false,"openAccessPdf":"https://www.ncbi.nlm.nih.gov/pmc/articles/PMC9833930/pdf/","citationCount":"2","resultStr":null,"platform":"Semanticscholar","paperid":null,"PeriodicalName":"Journal of Transplantation","FirstCategoryId":"1085","ListUrlMain":"https://doi.org/10.1155/2023/7915781","RegionNum":0,"RegionCategory":null,"ArticlePicture":[],"TitleCN":null,"AbstractTextCN":null,"PMCID":null,"EPubDate":"","PubModel":"","JCR":"Q3","JCRName":"SURGERY","Score":null,"Total":0}
引用次数: 2
Abstract
Background: Nonadherence to immunosuppression in liver transplant recipients (LTRs) leads to deterioration in health outcomes. Once-dailyextended-release tacrolimus (TAC-ER) may improve adherence when compared to twice-dailyimmediate-release tacrolimus (TAC-IR).
Methods: We conducted a randomized controlled study to evaluate medication adherence, clinical efficacy, and safety of TAC-ER in stable LTR. All patients >18 years who underwent liver transplantation before 6 months were eligible. Patients were randomized 1 : 1 to continued TAC-IR or conversion to TAC-ER. The primary outcome was change in medication adherence from baseline to 9 months, assessed using BAASIS. Secondary outcomes were tacrolimus trough levels, safety, and quality of life.
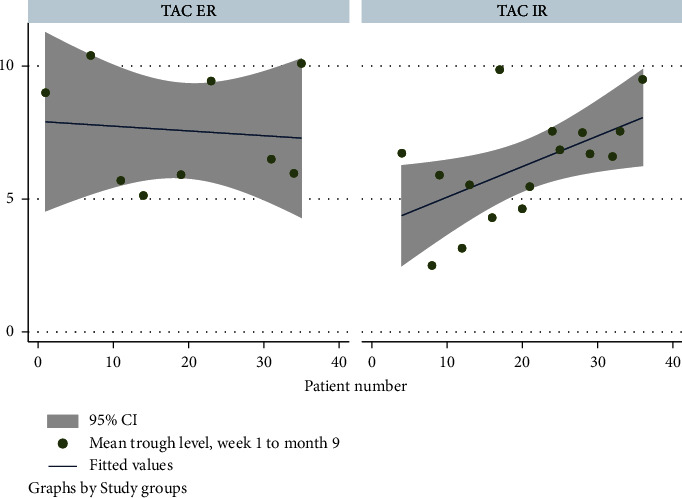
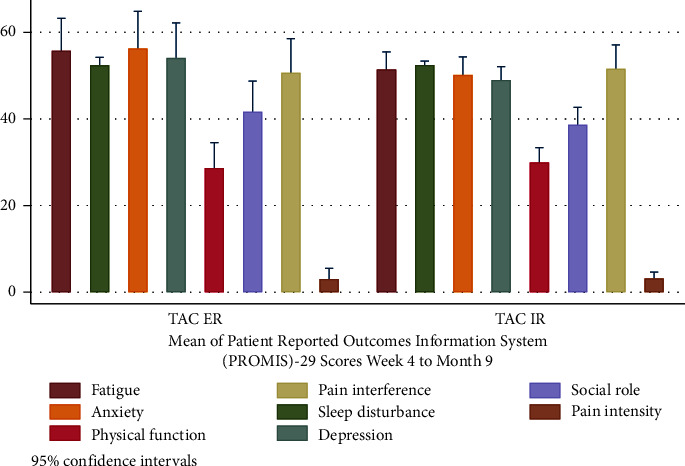
Results: Thirty-one patients were consented and randomized to either of the two groups: conversion to TAC-ER (n = 15) or continued TAC-IR (n = 16). Six patients in the TAC-ER group withdrew after randomization due to apprehension about switching medication (n = 2), unwillingness to travel (n = 2), and increased liver tests after conversion (n = 2, both were acute rejections despite therapeutic tacrolimus levels and were considered unrelated to TAC-ER). We compared the results of nine patients in the TAC-ER group that completed the study with those of sixteen in the TAC-IR group. At baseline, there was no difference in tacrolimus trough levels between groups. Improved adherence was observed in the TAC-ER group as 100% of patients reported at least one period of full adherence during the study period (100% vs. 62.6%, p = 0.035). Tacrolimus trough levels and liver tests were comparable between groups throughout the study. There were no differences in eGFR, HbA1c, or QoL between the groups.
Conclusion: TAC-ER improved medication adherence while maintaining comparable trough levels, liver function, and QoL as TAC-IR in LTR.

 求助内容:
求助内容: 应助结果提醒方式:
应助结果提醒方式:


