Matthew T Clark, Danielle A Rankin, Lauren S Peetluk, Alisa Gotte, Alison Herndon, William McEachern, Andrew Smith, Daniel E Clark, Edward Hardison, Adam J Esbenshade, Anna Patrick, Natasha B Halasa, James A Connelly, Sophie E Katz
{"title":"A Diagnostic Prediction Model to Distinguish Multisystem Inflammatory Syndrome in Children.","authors":"Matthew T Clark, Danielle A Rankin, Lauren S Peetluk, Alisa Gotte, Alison Herndon, William McEachern, Andrew Smith, Daniel E Clark, Edward Hardison, Adam J Esbenshade, Anna Patrick, Natasha B Halasa, James A Connelly, Sophie E Katz","doi":"10.1002/acr2.11509","DOIUrl":null,"url":null,"abstract":"<p><strong>Objective: </strong>Features of multisystem inflammatory syndrome in children (MIS-C) overlap with other syndromes, making the diagnosis difficult for clinicians. We aimed to compare clinical differences between patients with and without clinical MIS-C diagnosis and develop a diagnostic prediction model to assist clinicians in identification of patients with MIS-C within the first 24 hours of hospital presentation.</p><p><strong>Methods: </strong>A cohort of 127 patients (<21 years) were admitted to an academic children's hospital and evaluated for MIS-C. The primary outcome measure was MIS-C diagnosis at Vanderbilt University Medical Center. Clinical, laboratory, and cardiac features were extracted from the medical record, compared among groups, and selected a priori to identify candidate predictors. Final predictors were identified through a logistic regression model with bootstrapped backward selection in which only variables selected in more than 80% of 500 bootstraps were included in the final model.</p><p><strong>Results: </strong>Of 127 children admitted to our hospital with concern for MIS-C, 45 were clinically diagnosed with MIS-C and 82 were diagnosed with alternative diagnoses. We found a model with four variables-the presence of hypotension and/or fluid resuscitation, abdominal pain, new rash, and the value of serum sodium-showed excellent discrimination (concordance index 0.91; 95% confidence interval: 0.85-0.96) and good calibration in identifying patients with MIS-C.</p><p><strong>Conclusion: </strong>A diagnostic prediction model with early clinical and laboratory features shows excellent discrimination and may assist clinicians in distinguishing patients with MIS-C. This model will require external and prospective validation prior to widespread use.</p>","PeriodicalId":7084,"journal":{"name":"ACR Open Rheumatology","volume":"4 12","pages":"1050-1059"},"PeriodicalIF":0.0000,"publicationDate":"2022-12-01","publicationTypes":"Journal Article","fieldsOfStudy":null,"isOpenAccess":false,"openAccessPdf":"https://ftp.ncbi.nlm.nih.gov/pub/pmc/oa_pdf/8f/99/ACR2-4-1050.PMC9746665.pdf","citationCount":"0","resultStr":null,"platform":"Semanticscholar","paperid":null,"PeriodicalName":"ACR Open Rheumatology","FirstCategoryId":"1085","ListUrlMain":"https://doi.org/10.1002/acr2.11509","RegionNum":0,"RegionCategory":null,"ArticlePicture":[],"TitleCN":null,"AbstractTextCN":null,"PMCID":null,"EPubDate":"2022/11/1 0:00:00","PubModel":"Epub","JCR":"","JCRName":"","Score":null,"Total":0}
引用次数: 0
Abstract
Objective: Features of multisystem inflammatory syndrome in children (MIS-C) overlap with other syndromes, making the diagnosis difficult for clinicians. We aimed to compare clinical differences between patients with and without clinical MIS-C diagnosis and develop a diagnostic prediction model to assist clinicians in identification of patients with MIS-C within the first 24 hours of hospital presentation.
Methods: A cohort of 127 patients (<21 years) were admitted to an academic children's hospital and evaluated for MIS-C. The primary outcome measure was MIS-C diagnosis at Vanderbilt University Medical Center. Clinical, laboratory, and cardiac features were extracted from the medical record, compared among groups, and selected a priori to identify candidate predictors. Final predictors were identified through a logistic regression model with bootstrapped backward selection in which only variables selected in more than 80% of 500 bootstraps were included in the final model.
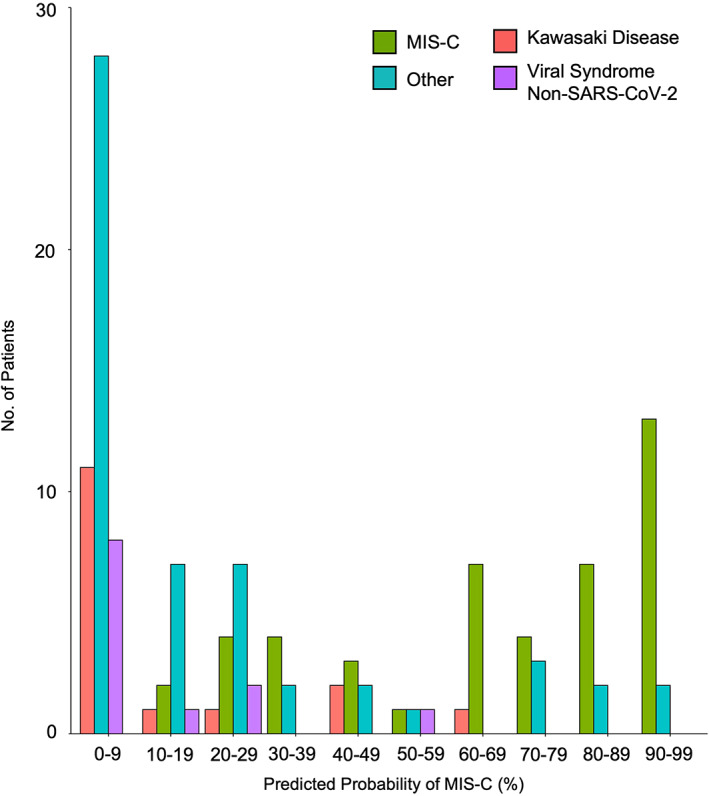
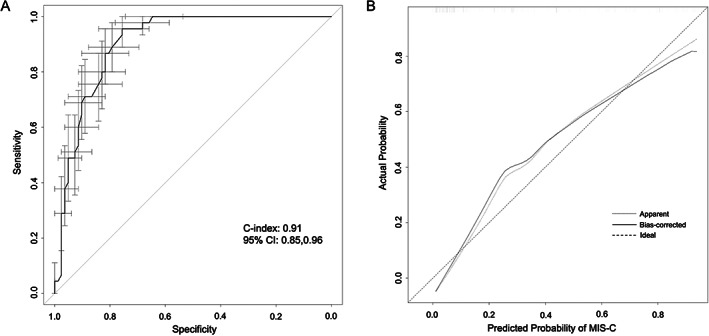
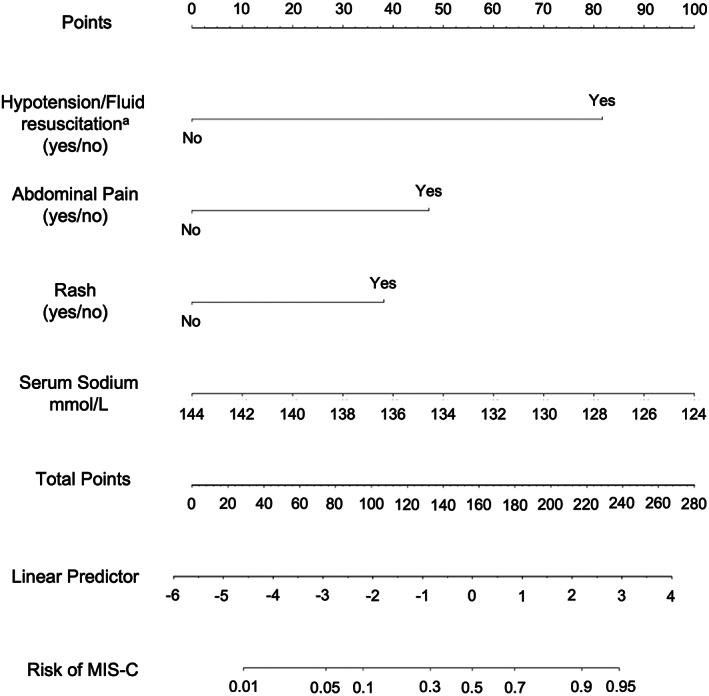
Results: Of 127 children admitted to our hospital with concern for MIS-C, 45 were clinically diagnosed with MIS-C and 82 were diagnosed with alternative diagnoses. We found a model with four variables-the presence of hypotension and/or fluid resuscitation, abdominal pain, new rash, and the value of serum sodium-showed excellent discrimination (concordance index 0.91; 95% confidence interval: 0.85-0.96) and good calibration in identifying patients with MIS-C.
Conclusion: A diagnostic prediction model with early clinical and laboratory features shows excellent discrimination and may assist clinicians in distinguishing patients with MIS-C. This model will require external and prospective validation prior to widespread use.

 求助内容:
求助内容: 应助结果提醒方式:
应助结果提醒方式:


