Nathalie Wilmsen, Hanno Pijl, Willem Geerlings, Gerjan Navis
{"title":"Retrospective analysis on the effect of Reverse Diabetes2 Now on kidney function in patients with type 2 diabetes with impaired kidney function.","authors":"Nathalie Wilmsen, Hanno Pijl, Willem Geerlings, Gerjan Navis","doi":"10.1136/bmjnph-2021-000397","DOIUrl":null,"url":null,"abstract":"<p><strong>Objective: </strong>Type 2 diabetes is one of the main causes of kidney damage. Recent intervention studies suggest that the progression of type 2 diabetes can be halted, or even brought into remission by lifestyle interventions. In a pragmatic trial, the Reverse Diabetes2 Now programme (RD2N, NL: Keer Diabetes2 Om), a multicomponent lifestyle intervention, reduced the need for bloodglucose lowering medications up to 24 months.</p><p><strong>Research design and methods: </strong>Here, we retrospectively investigate the effect of RD2N on markers of kidney function in patients selected for impaired kidney function at baseline (eGFR <70 mL/min/1.73 m<sup>2</sup> (n=45). Baseline data were retrieved from the intervention database and follow-up data on renal markers were collected from routine medical records. Wilcoxon non-parametric tests were used to assess changes over 6 and 12 months.</p><p><strong>Results: </strong>After 6 months median eGFR increased significantly from 62.0 (IQR 55.5-65.0) to 69.0 (IQR 55.0-76.5) mL/min/1.73 m<sup>2</sup> (p=0.002). Median albumin/creatinine ratio (n=26) remained within the normal range (<3 mg/mmol). The effect on eGFR was similar after exclusion of patients in whom medication was changed (median eGFR 62.0 ((IQR 59.5-66.0) to 69.0 (IQR 60.0-77.0) mL/min/1.73 m<sup>2</sup>, p=0.006, n=29), suggesting that the effect on eGFR is not related to medication changes. At 12 months, eGFR was not significantly changed (n=22, median eGFR 63.5 mL/min/1.73 m<sup>2</sup> (IQR 58.5-71.0), p=0.067).</p><p><strong>Conclusions: </strong>The retrospective nature of this study and the despite guidelines limited availability of renal markers in routine type 2 diabetes care are limiting. Nevertheless, these data support a favourable effect of RD2N on renal function. Further research, with proper documentation of renal function, urinary protein excretion and dietary intake, is needed to substantiate these results, ideally in a large-scale prospective cohort study.</p>","PeriodicalId":72435,"journal":{"name":"","volume":"5 2","pages":"271-276"},"PeriodicalIF":0.0,"publicationDate":"2022-12-01","publicationTypes":"Journal Article","fieldsOfStudy":null,"isOpenAccess":false,"openAccessPdf":"https://ftp.ncbi.nlm.nih.gov/pub/pmc/oa_pdf/34/7c/bmjnph-2021-000397.PMC9813621.pdf","citationCount":"0","resultStr":null,"platform":"Semanticscholar","paperid":null,"PeriodicalName":"","FirstCategoryId":"1085","ListUrlMain":"https://doi.org/10.1136/bmjnph-2021-000397","RegionNum":0,"RegionCategory":null,"ArticlePicture":[],"TitleCN":null,"AbstractTextCN":null,"PMCID":null,"EPubDate":"","PubModel":"","JCR":"","JCRName":"","Score":null,"Total":0}
引用次数: 0
Abstract
Objective: Type 2 diabetes is one of the main causes of kidney damage. Recent intervention studies suggest that the progression of type 2 diabetes can be halted, or even brought into remission by lifestyle interventions. In a pragmatic trial, the Reverse Diabetes2 Now programme (RD2N, NL: Keer Diabetes2 Om), a multicomponent lifestyle intervention, reduced the need for bloodglucose lowering medications up to 24 months.
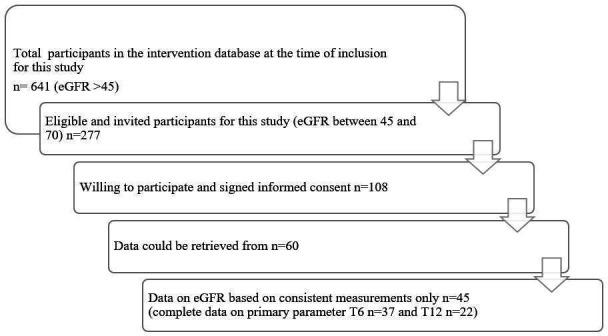
Research design and methods: Here, we retrospectively investigate the effect of RD2N on markers of kidney function in patients selected for impaired kidney function at baseline (eGFR <70 mL/min/1.73 m2 (n=45). Baseline data were retrieved from the intervention database and follow-up data on renal markers were collected from routine medical records. Wilcoxon non-parametric tests were used to assess changes over 6 and 12 months.
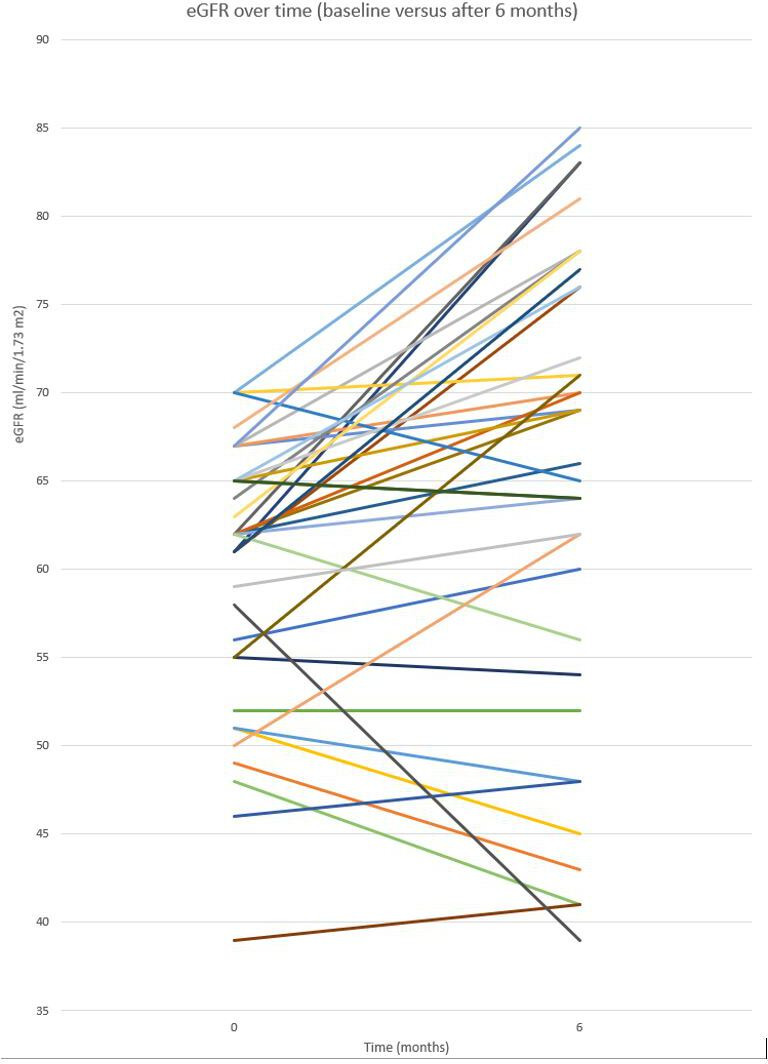
Results: After 6 months median eGFR increased significantly from 62.0 (IQR 55.5-65.0) to 69.0 (IQR 55.0-76.5) mL/min/1.73 m2 (p=0.002). Median albumin/creatinine ratio (n=26) remained within the normal range (<3 mg/mmol). The effect on eGFR was similar after exclusion of patients in whom medication was changed (median eGFR 62.0 ((IQR 59.5-66.0) to 69.0 (IQR 60.0-77.0) mL/min/1.73 m2, p=0.006, n=29), suggesting that the effect on eGFR is not related to medication changes. At 12 months, eGFR was not significantly changed (n=22, median eGFR 63.5 mL/min/1.73 m2 (IQR 58.5-71.0), p=0.067).
Conclusions: The retrospective nature of this study and the despite guidelines limited availability of renal markers in routine type 2 diabetes care are limiting. Nevertheless, these data support a favourable effect of RD2N on renal function. Further research, with proper documentation of renal function, urinary protein excretion and dietary intake, is needed to substantiate these results, ideally in a large-scale prospective cohort study.
 求助内容:
求助内容: 应助结果提醒方式:
应助结果提醒方式:


