{"title":"[Panhypopituitarism as the first manifestation of sarcoidosis: case report].","authors":"Yu A Ukhanova, I A Ilovayskaya, S A Terpigorev","doi":"10.14341/probl13115","DOIUrl":null,"url":null,"abstract":"<p><p>Sarcoidosis is a systemic inflammatory disease of unknown etiology characterized by the formation of noncaseating granulomas in various organs and tissues and the activation of T-cells at the site of granulomatous inflammation with the release of various chemokines and cytokines [1]. The incidence on average ranges from 10 to 20 per 100,000 population [2]. Most often in patients with sarcoidosis, lesions of the lungs and intrathoracic lymph nodes are detected. Significantly less often (in about 5-20% of patients) damage to the nervous system is noted [6,7,9]. In 9-18% of patients with neurosarcoidosis, involvement of the pituitary gland, pituitary infundibulum and hypothalamus is found, which is manifested by a variety of clinical symptoms [8,10]. We observed a patient with sarcoidosis whose disease debuted with clinical symptoms of hypogonadism, followed by the development of signs of secondary hypothyroidism, adrenal insufficiency, and diabetes insipidus, which was initially regarded as panhypopituitarism against the background of a hypothalamic lesion of unknown origin. Later, additional examination revealed signs of intrathoracic lymphadenopathy and focal changes in the lung parenchyma on CT, as well as skin lesions. Despite the biochemical compensation of hypopituitarism, the clinical efficacy of hormonal therapy with cabergoline, testosterone, hydrocortisone and levothyroxine sodium was insufficient, and the patient's condition improved after the addition of immunosuppressive and anti-inflammatory therapy with methotrexate and methylprednisolone.</p>","PeriodicalId":20433,"journal":{"name":"Problemy endokrinologii","volume":"68 4","pages":"46-51"},"PeriodicalIF":0.0000,"publicationDate":"2022-06-15","publicationTypes":"Journal Article","fieldsOfStudy":null,"isOpenAccess":false,"openAccessPdf":"https://www.ncbi.nlm.nih.gov/pmc/articles/PMC9762432/pdf/","citationCount":"0","resultStr":null,"platform":"Semanticscholar","paperid":null,"PeriodicalName":"Problemy endokrinologii","FirstCategoryId":"1085","ListUrlMain":"https://doi.org/10.14341/probl13115","RegionNum":0,"RegionCategory":null,"ArticlePicture":[],"TitleCN":null,"AbstractTextCN":null,"PMCID":null,"EPubDate":"","PubModel":"","JCR":"Q4","JCRName":"Medicine","Score":null,"Total":0}
引用次数: 0
Abstract
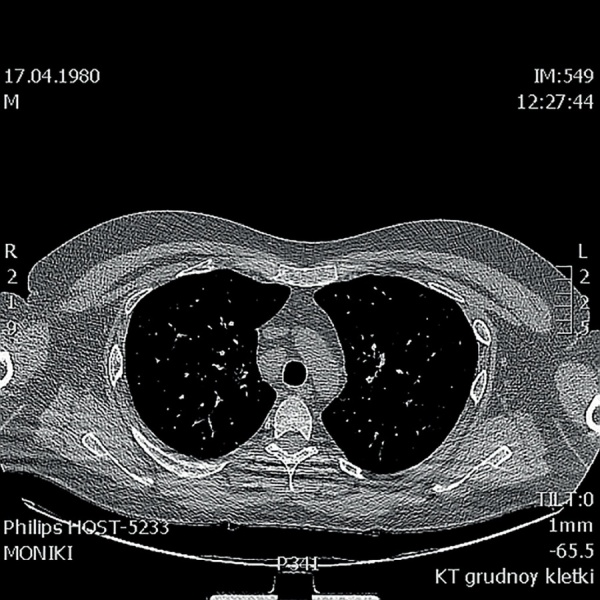
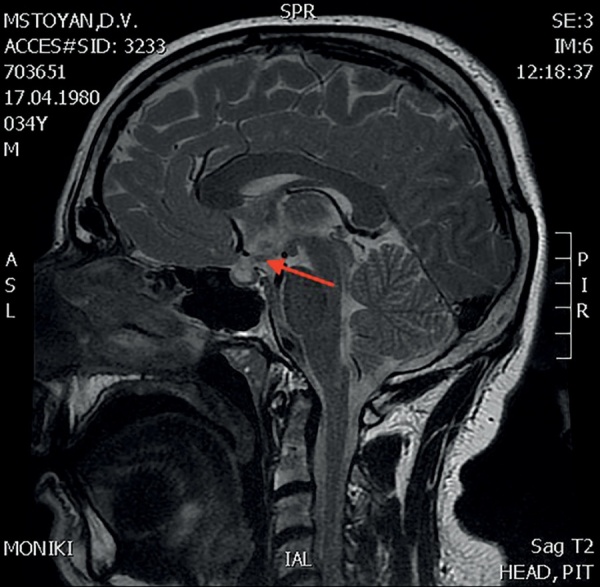
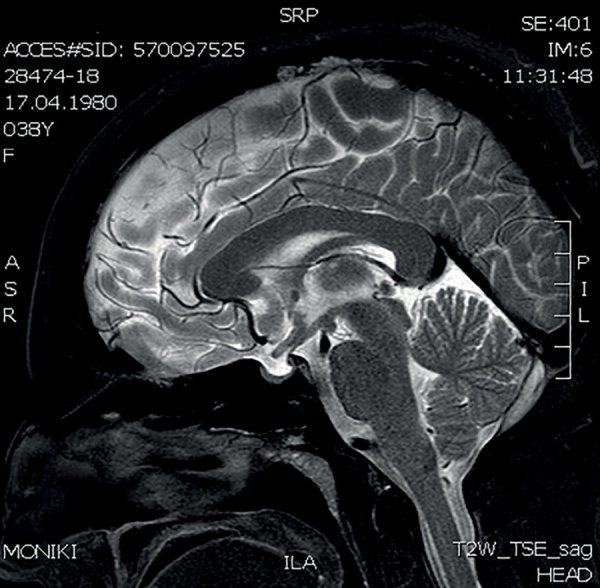
Sarcoidosis is a systemic inflammatory disease of unknown etiology characterized by the formation of noncaseating granulomas in various organs and tissues and the activation of T-cells at the site of granulomatous inflammation with the release of various chemokines and cytokines [1]. The incidence on average ranges from 10 to 20 per 100,000 population [2]. Most often in patients with sarcoidosis, lesions of the lungs and intrathoracic lymph nodes are detected. Significantly less often (in about 5-20% of patients) damage to the nervous system is noted [6,7,9]. In 9-18% of patients with neurosarcoidosis, involvement of the pituitary gland, pituitary infundibulum and hypothalamus is found, which is manifested by a variety of clinical symptoms [8,10]. We observed a patient with sarcoidosis whose disease debuted with clinical symptoms of hypogonadism, followed by the development of signs of secondary hypothyroidism, adrenal insufficiency, and diabetes insipidus, which was initially regarded as panhypopituitarism against the background of a hypothalamic lesion of unknown origin. Later, additional examination revealed signs of intrathoracic lymphadenopathy and focal changes in the lung parenchyma on CT, as well as skin lesions. Despite the biochemical compensation of hypopituitarism, the clinical efficacy of hormonal therapy with cabergoline, testosterone, hydrocortisone and levothyroxine sodium was insufficient, and the patient's condition improved after the addition of immunosuppressive and anti-inflammatory therapy with methotrexate and methylprednisolone.
期刊介绍:
Since 1955 the “Problems of Endocrinology” (or “Problemy Endocrinologii”) Journal publishes timely articles, balancing both clinical and experimental research, case reports, reviews and lectures on pressing problems of endocrinology. The Journal is aimed to the most topical issues of endocrinology: to chemical structure, biosynthesis and metabolism of hormones, the mechanism of their action at cellular and molecular level; pathogenesis and to clinic of the endocrine diseases, new methods of their diagnostics and treatment. The Journal: features original national and foreign research articles, reflecting world endocrinology development; issues thematic editions on specific areas; publishes chronicle of major international congress sessions and workshops on endocrinology, as well as state-of-the-art guidelines; is intended for scientists, endocrinologists diabetologists and specialists of allied trade, general practitioners, family physicians and pediatrics.

 求助内容:
求助内容: 应助结果提醒方式:
应助结果提醒方式:


