Cost Utility of Supporting Family-Based Care to Prevent HIV and Deaths among Orphaned and Separated Children in East Africa: A Markov Model-Based Simulation.
Marta Wilson-Barthes, Paula Braitstein, Allison DeLong, David Ayuku, Lukoye Atwoli, Edwin Sang, Omar Galárraga
{"title":"Cost Utility of Supporting Family-Based Care to Prevent HIV and Deaths among Orphaned and Separated Children in East Africa: A Markov Model-Based Simulation.","authors":"Marta Wilson-Barthes, Paula Braitstein, Allison DeLong, David Ayuku, Lukoye Atwoli, Edwin Sang, Omar Galárraga","doi":"10.1177/23814683221143782","DOIUrl":null,"url":null,"abstract":"<p><p><b>Purpose.</b> Strengthening family-based care is a key policy response to the more than 15 million orphaned and separated children who have lost 1 or both parents in sub-Saharan Africa. This analysis estimated the cost-effectiveness of family-based care environments for preventing HIV and death in this population. <b>Design.</b> We developed a time-homogeneous Markov model to simulate the incremental cost per disability-adjusted life year (DALY) averted by supporting family-based environments caring for orphaned and separated children in western Kenya. Model parameters were based on data from the longitudinal OSCAR's Health and Well-Being Project and published literature. We used a societal perspective, annual cycle length, and 3% discount rate. Incremental cost-effectiveness ratios were simulated over 5- to 15-y horizons, comparing family-based settings to street-based \"self-care.\" Parameter uncertainty was addressed via deterministic and probabilistic sensitivity analyses. <b>Results.</b> Under base-case assumptions, family-based environments prevented 422 HIV infections and 298 deaths in a simulated cohort of 1,000 individuals over 10 y. Compared with street-based self-care, family-based care had an incremental cost of $2,528 per DALY averted (95% confidence interval [CI]: 1,798, 2,599) and $2,355 per quality-adjusted life year gained (95% CI: 1,667, 2,413). The probability of family-based care being highly cost-effective was >80% at a willingness-to-pay (WTP) threshold of $2,250/DALY averted. Households receiving government cash transfers had minimally higher cost-effectiveness ratios than households without cash transfers but were still cost-effective at a WTP threshold of twice Kenya's GDP per capita. <b>Conclusions.</b> Compared with the status quo of street-based self-care, family-based environments offer a cost-effective approach for preventing HIV and death among orphaned children in lower-middle income countries. Decision makers should consider increasing resources to these environments in tandem with social protection programs.</p><p><strong>Highlights: </strong>UNICEF and more than 200 other international organizations endorsed efforts to redirect services toward family-based care as part of the 2019 UN Resolution on the Rights of the Child; yet this study is one of the first to quantify the cost-effectiveness of family-based care environments serving some of the world's most vulnerable children.This health economic modeling analysis found that family-based environments would prevent 422 HIV infections and 298 deaths in a cohort of 1,000 orphaned and separated children over a 10-y time horizon.Compared with street-based \"self-care,\" family-based care resulted in an incremental cost of $2,528 per DALY averted (95% CI: 1,798, 2,599) and $2,355 per quality-adjusted life year gained (95% CI: 1,667, 2,413) after 10 y.Annual per-child expenditures for children living in family-based care environments in sub-Saharan Africa could potentially be increased by at least 25% and remain highly cost-effective.</p>","PeriodicalId":36567,"journal":{"name":"MDM Policy and Practice","volume":"7 2","pages":"23814683221143782"},"PeriodicalIF":1.7000,"publicationDate":"2022-07-01","publicationTypes":"Journal Article","fieldsOfStudy":null,"isOpenAccess":false,"openAccessPdf":"https://ftp.ncbi.nlm.nih.gov/pub/pmc/oa_pdf/04/8a/10.1177_23814683221143782.PMC9806382.pdf","citationCount":"0","resultStr":null,"platform":"Semanticscholar","paperid":null,"PeriodicalName":"MDM Policy and Practice","FirstCategoryId":"1085","ListUrlMain":"https://doi.org/10.1177/23814683221143782","RegionNum":0,"RegionCategory":null,"ArticlePicture":[],"TitleCN":null,"AbstractTextCN":null,"PMCID":null,"EPubDate":"","PubModel":"","JCR":"Q3","JCRName":"HEALTH CARE SCIENCES & SERVICES","Score":null,"Total":0}
引用次数: 0
Abstract
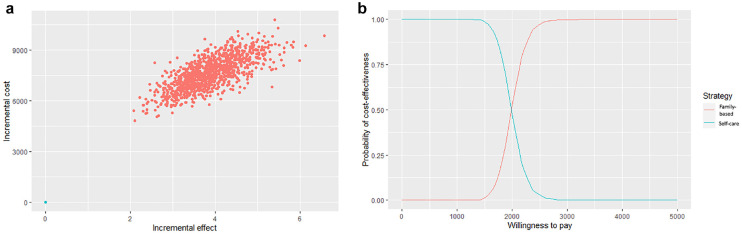
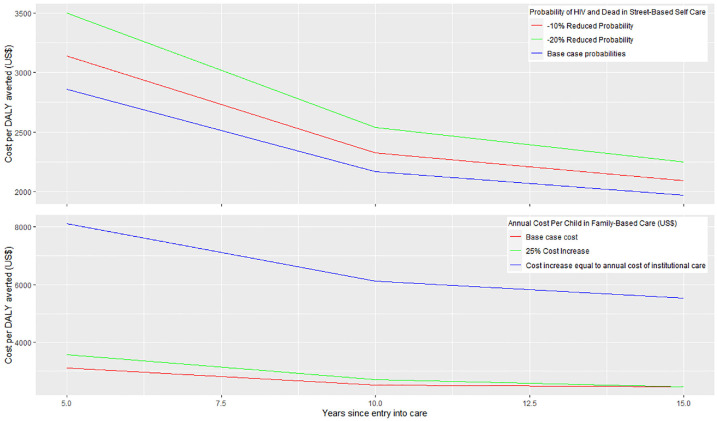
Purpose. Strengthening family-based care is a key policy response to the more than 15 million orphaned and separated children who have lost 1 or both parents in sub-Saharan Africa. This analysis estimated the cost-effectiveness of family-based care environments for preventing HIV and death in this population. Design. We developed a time-homogeneous Markov model to simulate the incremental cost per disability-adjusted life year (DALY) averted by supporting family-based environments caring for orphaned and separated children in western Kenya. Model parameters were based on data from the longitudinal OSCAR's Health and Well-Being Project and published literature. We used a societal perspective, annual cycle length, and 3% discount rate. Incremental cost-effectiveness ratios were simulated over 5- to 15-y horizons, comparing family-based settings to street-based "self-care." Parameter uncertainty was addressed via deterministic and probabilistic sensitivity analyses. Results. Under base-case assumptions, family-based environments prevented 422 HIV infections and 298 deaths in a simulated cohort of 1,000 individuals over 10 y. Compared with street-based self-care, family-based care had an incremental cost of $2,528 per DALY averted (95% confidence interval [CI]: 1,798, 2,599) and $2,355 per quality-adjusted life year gained (95% CI: 1,667, 2,413). The probability of family-based care being highly cost-effective was >80% at a willingness-to-pay (WTP) threshold of $2,250/DALY averted. Households receiving government cash transfers had minimally higher cost-effectiveness ratios than households without cash transfers but were still cost-effective at a WTP threshold of twice Kenya's GDP per capita. Conclusions. Compared with the status quo of street-based self-care, family-based environments offer a cost-effective approach for preventing HIV and death among orphaned children in lower-middle income countries. Decision makers should consider increasing resources to these environments in tandem with social protection programs.
Highlights: UNICEF and more than 200 other international organizations endorsed efforts to redirect services toward family-based care as part of the 2019 UN Resolution on the Rights of the Child; yet this study is one of the first to quantify the cost-effectiveness of family-based care environments serving some of the world's most vulnerable children.This health economic modeling analysis found that family-based environments would prevent 422 HIV infections and 298 deaths in a cohort of 1,000 orphaned and separated children over a 10-y time horizon.Compared with street-based "self-care," family-based care resulted in an incremental cost of $2,528 per DALY averted (95% CI: 1,798, 2,599) and $2,355 per quality-adjusted life year gained (95% CI: 1,667, 2,413) after 10 y.Annual per-child expenditures for children living in family-based care environments in sub-Saharan Africa could potentially be increased by at least 25% and remain highly cost-effective.


 求助内容:
求助内容: 应助结果提醒方式:
应助结果提醒方式:


