{"title":"A New Coronavirus Estimation Global Score for Predicting Mortality During Hospitalization in Patients with COVID-19.","authors":"Hesong Zeng, Xingwei He, Wanjun Liu, Jing Kan, Liqun He, Jinhe Zhao, Cynthia Chen, Junjie Zhang, Shaoliang Chen","doi":"10.1097/CD9.0000000000000052","DOIUrl":null,"url":null,"abstract":"<p><strong>Objective: </strong>Coronavirus disease 2019 (COVID-19) exists as a pandemic. Mortality during hospitalization is multifactorial, and there is urgent need for a risk stratification model to predict in-hospital death among COVID-19 patients. Here we aimed to construct a risk score system for early identification of COVID-19 patients at high probability of dying during in-hospital treatment.</p><p><strong>Methods: </strong>In this retrospective analysis, a total of 821 confirmed COVID-19 patients from 3 centers were assigned to developmental (<i>n</i> = 411, between January 14, 2020 and February 11, 2020) and validation (<i>n</i> = 410, between February 14, 2020 and March 13, 2020) groups. Based on demographic, symptomatic, and laboratory variables, a new Coronavirus estimation global (CORE-G) score for prediction of in-hospital death was established from the developmental group, and its performance was then evaluated in the validation group.</p><p><strong>Results: </strong>The CORE-G score consisted of 18 variables (5 demographics, 2 symptoms, and 11 laboratory measurements) with a sum of 69.5 points. Goodness-of-fit tests indicated that the model performed well in the developmental group (<i>H</i> = 3.210, <i>P</i> <i>=</i> 0.880), and it was well validated in the validation group (<i>H</i> = 6.948, <i>P</i> <i>=</i> 0.542). The areas under the receiver operating characteristic curves were 0.955 in the developmental group (sensitivity, 94.1%; specificity, 83.4%) and 0.937 in the validation group (sensitivity, 87.2%; specificity, 84.2%). The mortality rate was not significantly different between the developmental (<i>n</i> = 85,20.7%) and validation (<i>n</i> = 94, 22.9%, <i>P</i> <i>=</i> 0.608) groups.</p><p><strong>Conclusions: </strong>The CORE-G score provides an estimate of the risk of in-hospital death. This is the first step toward the clinical use of the CORE-G score for predicting outcome in COVID-19 patients.</p>","PeriodicalId":72524,"journal":{"name":"Cardiology discovery","volume":"2 2","pages":"69-76"},"PeriodicalIF":0.9000,"publicationDate":"2022-06-01","publicationTypes":"Journal Article","fieldsOfStudy":null,"isOpenAccess":false,"openAccessPdf":"https://ftp.ncbi.nlm.nih.gov/pub/pmc/oa_pdf/d8/33/cd9-2-69.PMC9749948.pdf","citationCount":"0","resultStr":null,"platform":"Semanticscholar","paperid":null,"PeriodicalName":"Cardiology discovery","FirstCategoryId":"1085","ListUrlMain":"https://doi.org/10.1097/CD9.0000000000000052","RegionNum":0,"RegionCategory":null,"ArticlePicture":[],"TitleCN":null,"AbstractTextCN":null,"PMCID":null,"EPubDate":"","PubModel":"","JCR":"","JCRName":"","Score":null,"Total":0}
引用次数: 0
Abstract
Objective: Coronavirus disease 2019 (COVID-19) exists as a pandemic. Mortality during hospitalization is multifactorial, and there is urgent need for a risk stratification model to predict in-hospital death among COVID-19 patients. Here we aimed to construct a risk score system for early identification of COVID-19 patients at high probability of dying during in-hospital treatment.
Methods: In this retrospective analysis, a total of 821 confirmed COVID-19 patients from 3 centers were assigned to developmental (n = 411, between January 14, 2020 and February 11, 2020) and validation (n = 410, between February 14, 2020 and March 13, 2020) groups. Based on demographic, symptomatic, and laboratory variables, a new Coronavirus estimation global (CORE-G) score for prediction of in-hospital death was established from the developmental group, and its performance was then evaluated in the validation group.
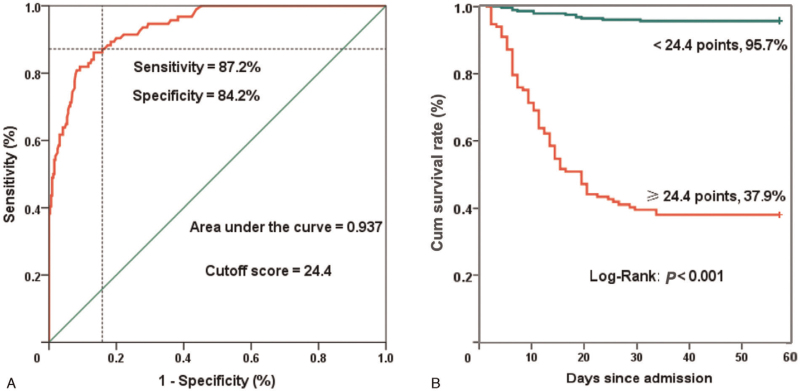
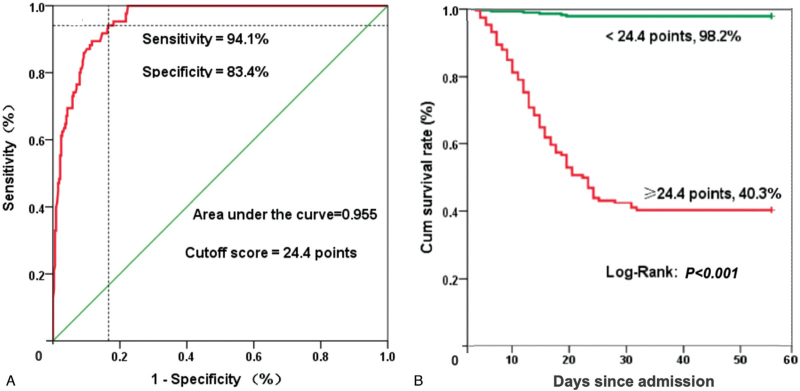
Results: The CORE-G score consisted of 18 variables (5 demographics, 2 symptoms, and 11 laboratory measurements) with a sum of 69.5 points. Goodness-of-fit tests indicated that the model performed well in the developmental group (H = 3.210, P= 0.880), and it was well validated in the validation group (H = 6.948, P= 0.542). The areas under the receiver operating characteristic curves were 0.955 in the developmental group (sensitivity, 94.1%; specificity, 83.4%) and 0.937 in the validation group (sensitivity, 87.2%; specificity, 84.2%). The mortality rate was not significantly different between the developmental (n = 85,20.7%) and validation (n = 94, 22.9%, P= 0.608) groups.
Conclusions: The CORE-G score provides an estimate of the risk of in-hospital death. This is the first step toward the clinical use of the CORE-G score for predicting outcome in COVID-19 patients.

 求助内容:
求助内容: 应助结果提醒方式:
应助结果提醒方式:


