{"title":"Initial Experience of Hybrid Technique in Robot-Assisted Intracorporeal Ileal Conduit.","authors":"Shugo Yajima, Yasukazu Nakanishi, Yousuke Umino, Naoya Ookubo, Kenji Tanabe, Madoka Kataoka, Hitoshi Masuda","doi":"10.5152/tud.2022.22125","DOIUrl":null,"url":null,"abstract":"<p><strong>Objective: </strong>This study was designed to describe our hybrid approach to intracorporeal urinary diversion and evaluate surgical experience during initial induction.</p><p><strong>Material and methods: </strong>Clinical data from 38 patients with bladder cancer undergoing robot-assisted radical cystectomy with ileal conduit hybrid approach to intracorporeal urinary diversion at our institution between May 2020 and January 2022 were reviewed. The hybrid approach to intracorporeal urinary diversion pro cedure involved the following: radical cystectomy, removing a specimen through a 4- to 6-cm skin incision, harvesting an ileal conduit, redocking the robot, and uretero-uretero anastomosis. The relationship between surgical experience and operative time and a Clavien-Dindo classification of grade >3 was evaluated.</p><p><strong>Results: </strong>Of the 38 patients, 30 (79%) were male, and the median age was 75 years (interquartile range, 71-80 years). The total operative time was 384 minutes (interquartile range, 348-409 minutes). The estimated blood loss was 244 mL (interquartile range, 124-445 mL). No bowel injuries or conversions to laparoscopy or laparotomy were encountered. High-grade postoperative complications (Clavien-Dindo classification grade > 3) occurred in 7 cases (19%). The overall 90-day readmission rate following discharge after surgery was 5%. The relationship between surgical experience and operative time was nonlinear. A plateau was not reached in all 38 patients.</p><p><strong>Conclusion: </strong>Our hybrid approach to intracorporeal urinary diversion technique can be accomplished safely with acceptable operative times, even with little surgical experience. This procedure might be a safe treat ment option that is relatively easy to perform, particularly in an institution that has not yet introduced intra corporeal urinary diversion. Future randomized trials with larger samples and longer follow-up periods are required to confirm our findings.</p>","PeriodicalId":23366,"journal":{"name":"Turkish journal of urology","volume":"48 6","pages":"415-422"},"PeriodicalIF":1.1000,"publicationDate":"2022-11-01","publicationTypes":"Journal Article","fieldsOfStudy":null,"isOpenAccess":false,"openAccessPdf":"https://www.ncbi.nlm.nih.gov/pmc/articles/PMC9797707/pdf/","citationCount":"0","resultStr":null,"platform":"Semanticscholar","paperid":null,"PeriodicalName":"Turkish journal of urology","FirstCategoryId":"1085","ListUrlMain":"https://doi.org/10.5152/tud.2022.22125","RegionNum":0,"RegionCategory":null,"ArticlePicture":[],"TitleCN":null,"AbstractTextCN":null,"PMCID":null,"EPubDate":"","PubModel":"","JCR":"Q4","JCRName":"UROLOGY & NEPHROLOGY","Score":null,"Total":0}
引用次数: 0
Abstract
Objective: This study was designed to describe our hybrid approach to intracorporeal urinary diversion and evaluate surgical experience during initial induction.
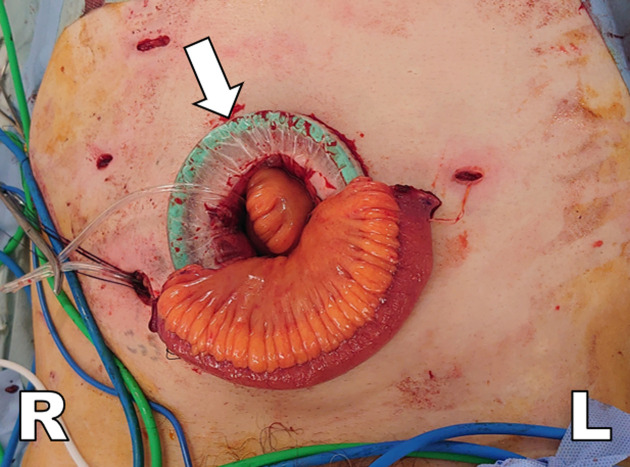
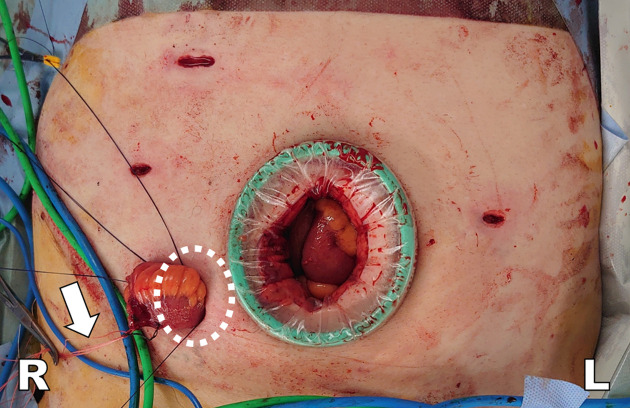
Material and methods: Clinical data from 38 patients with bladder cancer undergoing robot-assisted radical cystectomy with ileal conduit hybrid approach to intracorporeal urinary diversion at our institution between May 2020 and January 2022 were reviewed. The hybrid approach to intracorporeal urinary diversion pro cedure involved the following: radical cystectomy, removing a specimen through a 4- to 6-cm skin incision, harvesting an ileal conduit, redocking the robot, and uretero-uretero anastomosis. The relationship between surgical experience and operative time and a Clavien-Dindo classification of grade >3 was evaluated.
Results: Of the 38 patients, 30 (79%) were male, and the median age was 75 years (interquartile range, 71-80 years). The total operative time was 384 minutes (interquartile range, 348-409 minutes). The estimated blood loss was 244 mL (interquartile range, 124-445 mL). No bowel injuries or conversions to laparoscopy or laparotomy were encountered. High-grade postoperative complications (Clavien-Dindo classification grade > 3) occurred in 7 cases (19%). The overall 90-day readmission rate following discharge after surgery was 5%. The relationship between surgical experience and operative time was nonlinear. A plateau was not reached in all 38 patients.
Conclusion: Our hybrid approach to intracorporeal urinary diversion technique can be accomplished safely with acceptable operative times, even with little surgical experience. This procedure might be a safe treat ment option that is relatively easy to perform, particularly in an institution that has not yet introduced intra corporeal urinary diversion. Future randomized trials with larger samples and longer follow-up periods are required to confirm our findings.
期刊介绍:
The aim of the Turkish Journal of Urology is to contribute to the literature by publishing scientifically high-quality research articles as well as reviews, editorials, letters to the editor and case reports. The journal’s target audience includes, urology specialists, medical specialty fellows and other specialists and practitioners who are interested in the field of urology.


 求助内容:
求助内容: 应助结果提醒方式:
应助结果提醒方式:


