Initiation of iGlarLixi Versus Basal-Bolus Insulin in Adults With Type 2 Diabetes Advancing From Basal Insulin Therapy: The SoliComplex Real-World Study.
Kevin M Pantalone, Caroline Heller, Rosemarie Lajara, Elisheva Lew, Xuan Li, Terry Dex, C Rachel Kilpatrick
{"title":"Initiation of iGlarLixi Versus Basal-Bolus Insulin in Adults With Type 2 Diabetes Advancing From Basal Insulin Therapy: The SoliComplex Real-World Study.","authors":"Kevin M Pantalone, Caroline Heller, Rosemarie Lajara, Elisheva Lew, Xuan Li, Terry Dex, C Rachel Kilpatrick","doi":"10.2337/ds22-0064","DOIUrl":null,"url":null,"abstract":"<p><strong>Background: </strong>When type 2 diabetes is suboptimally controlled with basal insulin, prandial insulin injections are commonly added (i.e., a basal-bolus insulin regimen), which can increase treatment burden and hypoglycemia risk. The once-daily injectable iGlarLixi is an alternative treatment.</p><p><strong>Methods: </strong>This retrospective analysis of the U.S. Optum Clinformatics database compared outcomes in adults (≥18 years of age) with type 2 diabetes who previously received basal insulin and were newly initiated on iGlarLixi or basal-bolus insulin therapy. Cohorts were propensity score-matched in a 1:1 ratio on baseline characteristics, and imbalances were adjusted in multivariate analyses. Subgroup analyses were performed for people ≥65 years of age and those with a baseline A1C ≥9%. The primary end point was persistence with therapy at 12 months in the overall population. Secondary end points were treatment adherence, health care resource utilization (HCRU), costs, any hypoglycemia, and A1C change at 12 months.</p><p><strong>Results: </strong>Cohorts each comprised 1,070 participants. Treatment persistence at 12 months was statistically significantly higher for iGlarLixi versus basal-bolus insulin therapy (43.7 vs. 22.3%, hazard ratio 0.51, 95% CI 0.46-0.57, adjusted <i>P</i> <0.001). Adherence was numerically higher for iGlarLixi, and hypoglycemia events, HCRU, and costs were numerically lower for iGlarLixi. A1C reduction from baseline was slightly greater for basal-bolus insulin. Results for both subgroups (≥65 years of age and baseline A1C ≥9%) were similar to those of the overall population.</p><p><strong>Conclusion: </strong>In this observational study, initiation of once-daily iGlarLixi versus basal-bolus insulin was associated with higher persistence, lower hypoglycemia, and similar A1C reduction without increasing HCRU or costs regardless of age or A1C. iGlarLixi could be an alternative to basal-bolus insulin, particularly for older adults with type 2 diabetes who require treatment simplification with lower hypoglycemia risk.</p>","PeriodicalId":72797,"journal":{"name":"","volume":"36 3","pages":"253-263"},"PeriodicalIF":0.0,"publicationDate":"2023-01-01","publicationTypes":"Journal Article","fieldsOfStudy":null,"isOpenAccess":false,"openAccessPdf":"https://www.ncbi.nlm.nih.gov/pmc/articles/PMC10425231/pdf/","citationCount":"1","resultStr":null,"platform":"Semanticscholar","paperid":null,"PeriodicalName":"","FirstCategoryId":"1085","ListUrlMain":"https://doi.org/10.2337/ds22-0064","RegionNum":0,"RegionCategory":null,"ArticlePicture":[],"TitleCN":null,"AbstractTextCN":null,"PMCID":null,"EPubDate":"","PubModel":"","JCR":"","JCRName":"","Score":null,"Total":0}
引用次数: 1
Abstract
Background: When type 2 diabetes is suboptimally controlled with basal insulin, prandial insulin injections are commonly added (i.e., a basal-bolus insulin regimen), which can increase treatment burden and hypoglycemia risk. The once-daily injectable iGlarLixi is an alternative treatment.
Methods: This retrospective analysis of the U.S. Optum Clinformatics database compared outcomes in adults (≥18 years of age) with type 2 diabetes who previously received basal insulin and were newly initiated on iGlarLixi or basal-bolus insulin therapy. Cohorts were propensity score-matched in a 1:1 ratio on baseline characteristics, and imbalances were adjusted in multivariate analyses. Subgroup analyses were performed for people ≥65 years of age and those with a baseline A1C ≥9%. The primary end point was persistence with therapy at 12 months in the overall population. Secondary end points were treatment adherence, health care resource utilization (HCRU), costs, any hypoglycemia, and A1C change at 12 months.
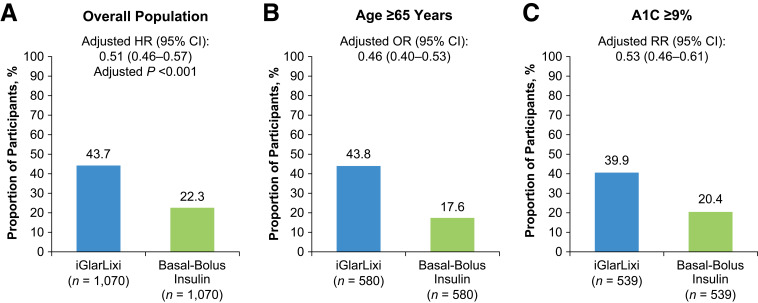
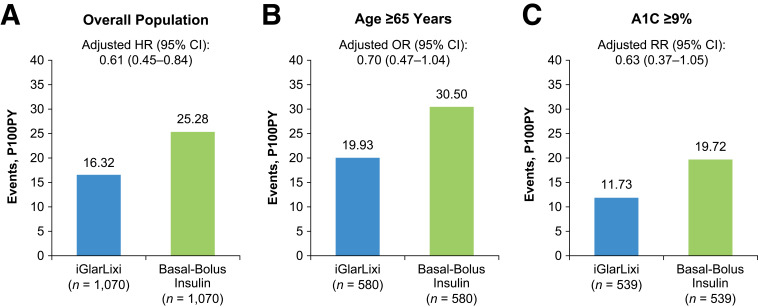
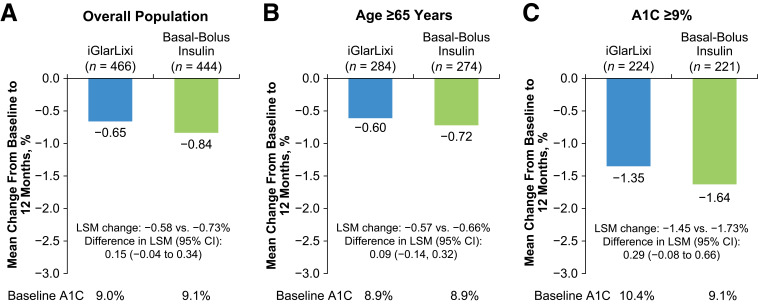
Results: Cohorts each comprised 1,070 participants. Treatment persistence at 12 months was statistically significantly higher for iGlarLixi versus basal-bolus insulin therapy (43.7 vs. 22.3%, hazard ratio 0.51, 95% CI 0.46-0.57, adjusted P <0.001). Adherence was numerically higher for iGlarLixi, and hypoglycemia events, HCRU, and costs were numerically lower for iGlarLixi. A1C reduction from baseline was slightly greater for basal-bolus insulin. Results for both subgroups (≥65 years of age and baseline A1C ≥9%) were similar to those of the overall population.
Conclusion: In this observational study, initiation of once-daily iGlarLixi versus basal-bolus insulin was associated with higher persistence, lower hypoglycemia, and similar A1C reduction without increasing HCRU or costs regardless of age or A1C. iGlarLixi could be an alternative to basal-bolus insulin, particularly for older adults with type 2 diabetes who require treatment simplification with lower hypoglycemia risk.
背景:当2型糖尿病在基础胰岛素控制下处于次优状态时,通常会增加餐前胰岛素注射(即基础胰岛素方案),这可能会增加治疗负担和低血糖风险。每日一次注射iGlarLixi是一种替代治疗方法。方法:对美国Optum Clinformatics数据库进行回顾性分析,比较了先前接受基础胰岛素治疗并新开始接受iGlarLixi或基础胰岛素治疗的2型糖尿病成人(≥18岁)的结局。队列在基线特征上按1:1的比例进行倾向评分匹配,并在多变量分析中调整不平衡。对≥65岁和基线A1C≥9%的患者进行亚组分析。主要终点是在总体人群中持续治疗12个月。次要终点是治疗依从性、卫生保健资源利用率(HCRU)、费用、任何低血糖和12个月时的A1C变化。结果:每个队列包括1,070名参与者。iGlarLixi治疗12个月时的治疗持久性比基础胰岛素治疗高(43.7 vs 22.3%,风险比0.51,95% CI 0.46-0.57,校正P)。结论:在这项观察性研究中,与基础胰岛素治疗相比,每日一次的iGlarLixi治疗与更高的持久性、更低的低血糖和类似的A1C降低相关,而不增加HCRU或成本,无论年龄或A1C。iGlarLixi可能是基础胰岛素的替代方案,特别是对于需要简化治疗并降低低血糖风险的老年2型糖尿病患者。
 求助内容:
求助内容: 应助结果提醒方式:
应助结果提醒方式:


