{"title":"Long short-term memory model identifies ARDS and in-hospital mortality in both non-COVID-19 and COVID-19 cohort.","authors":"Jen-Ting Chen, Rahil Mehrizi, Boudewijn Aasman, Michelle Ng Gong, Parsa Mirhaji","doi":"10.1136/bmjhci-2023-100782","DOIUrl":null,"url":null,"abstract":"<p><strong>Objective: </strong>To identify the risk of acute respiratory distress syndrome (ARDS) and in-hospital mortality using long short-term memory (LSTM) framework in a mechanically ventilated (MV) non-COVID-19 cohort and a COVID-19 cohort.</p><p><strong>Methods: </strong>We included MV ICU patients between 2017 and 2018 and reviewed patient records for ARDS and death. Using active learning, we enriched this cohort with MV patients from 2016 to 2019 (MV non-COVID-19, n=3905). We collected a second validation cohort of hospitalised patients with COVID-19 in 2020 (COVID+, n=5672). We trained an LSTM model using 132 structured features on the MV non-COVID-19 training cohort and validated on the MV non-COVID-19 validation and COVID-19 cohorts.</p><p><strong>Results: </strong>Applying LSTM (model score 0.9) on the MV non-COVID-19 validation cohort had a sensitivity of 86% and specificity of 57%. The model identified the risk of ARDS 10 hours before ARDS and 9.4 days before death. The sensitivity (70%) and specificity (84%) of the model on the COVID-19 cohort are lower than MV non-COVID-19 cohort. For the COVID-19 + cohort and MV COVID-19 + patients, the model identified the risk of in-hospital mortality 2.4 days and 1.54 days before death, respectively.</p><p><strong>Discussion: </strong>Our LSTM algorithm accurately and timely identified the risk of ARDS or death in MV non-COVID-19 and COVID+ patients. By alerting the risk of ARDS or death, we can improve the implementation of evidence-based ARDS management and facilitate goals-of-care discussions in high-risk patients.</p><p><strong>Conclusion: </strong>Using the LSTM algorithm in hospitalised patients identifies the risk of ARDS or death.</p>","PeriodicalId":9050,"journal":{"name":"BMJ Health & Care Informatics","volume":"30 1","pages":""},"PeriodicalIF":4.4000,"publicationDate":"2023-09-01","publicationTypes":"Journal Article","fieldsOfStudy":null,"isOpenAccess":false,"openAccessPdf":"https://ftp.ncbi.nlm.nih.gov/pub/pmc/oa_pdf/9d/16/bmjhci-2023-100782.PMC10503386.pdf","citationCount":"0","resultStr":null,"platform":"Semanticscholar","paperid":null,"PeriodicalName":"BMJ Health & Care Informatics","FirstCategoryId":"1085","ListUrlMain":"https://doi.org/10.1136/bmjhci-2023-100782","RegionNum":0,"RegionCategory":null,"ArticlePicture":[],"TitleCN":null,"AbstractTextCN":null,"PMCID":null,"EPubDate":"","PubModel":"","JCR":"Q1","JCRName":"HEALTH CARE SCIENCES & SERVICES","Score":null,"Total":0}
引用次数: 0
Abstract
Objective: To identify the risk of acute respiratory distress syndrome (ARDS) and in-hospital mortality using long short-term memory (LSTM) framework in a mechanically ventilated (MV) non-COVID-19 cohort and a COVID-19 cohort.
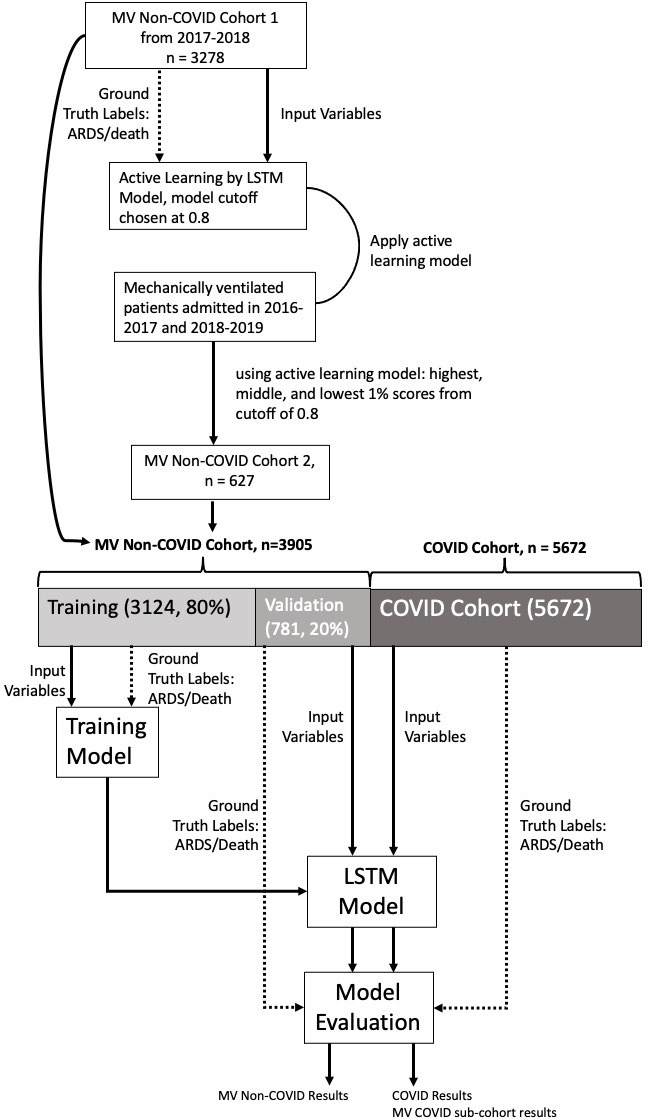
Methods: We included MV ICU patients between 2017 and 2018 and reviewed patient records for ARDS and death. Using active learning, we enriched this cohort with MV patients from 2016 to 2019 (MV non-COVID-19, n=3905). We collected a second validation cohort of hospitalised patients with COVID-19 in 2020 (COVID+, n=5672). We trained an LSTM model using 132 structured features on the MV non-COVID-19 training cohort and validated on the MV non-COVID-19 validation and COVID-19 cohorts.
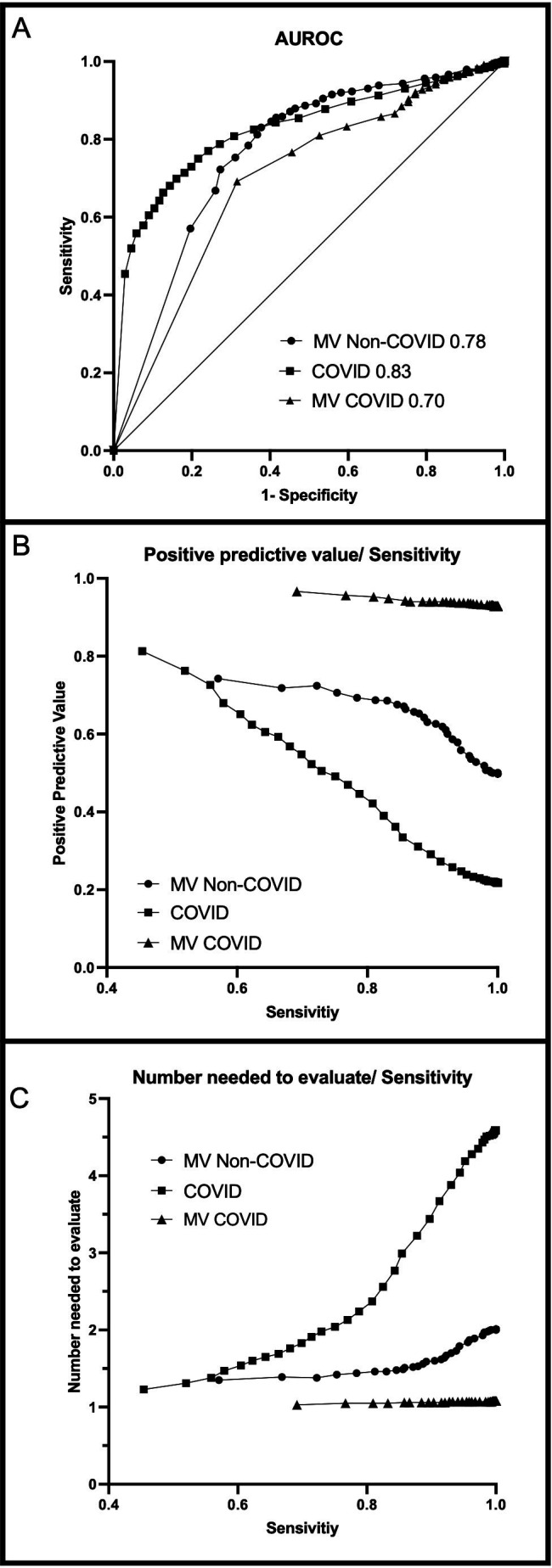
Results: Applying LSTM (model score 0.9) on the MV non-COVID-19 validation cohort had a sensitivity of 86% and specificity of 57%. The model identified the risk of ARDS 10 hours before ARDS and 9.4 days before death. The sensitivity (70%) and specificity (84%) of the model on the COVID-19 cohort are lower than MV non-COVID-19 cohort. For the COVID-19 + cohort and MV COVID-19 + patients, the model identified the risk of in-hospital mortality 2.4 days and 1.54 days before death, respectively.
Discussion: Our LSTM algorithm accurately and timely identified the risk of ARDS or death in MV non-COVID-19 and COVID+ patients. By alerting the risk of ARDS or death, we can improve the implementation of evidence-based ARDS management and facilitate goals-of-care discussions in high-risk patients.
Conclusion: Using the LSTM algorithm in hospitalised patients identifies the risk of ARDS or death.

 求助内容:
求助内容: 应助结果提醒方式:
应助结果提醒方式:


