Long-term patency of arteriovenous fistulas for hemodialysis: A decade's experience in a transplant unit
Abstract
Background
The heterogeneous quality of studies on arteriovenous fistulas outcome, with variable clinical settings and large variations in definitions of patency and failure rates, leads to frequent misinterpretations and overestimation of arteriovenous fistula patency. Hence, this study aimed to provide realistic and clinically relevant long-term arteriovenous fistula outcomes.
Methods
We retrospectively analyzed all autologous arteriovenous fistulas at our center over a 10-year period (2012–2022). Primary and secondary patency analysis was conducted using the Kaplan–Meier method; multivariate analysis of variance was used to detect outcome predictors. Vascular access-specific endpoints were defined according to the European guidelines on vascular access formation.
Findings
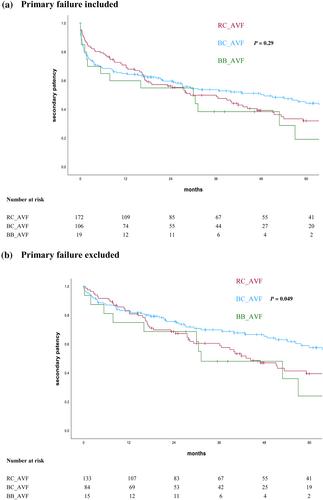
Of 312 arteriovenous fistulas, 57.5% (n = 181) were radio-cephalic (RC_AVF), 35.2% (n = 111) brachio-cephalic (BC_AVF), and 6.3% (n = 20) brachio-basilic (BB_AVF). 6, 12, and 24 months follow-up was available in 290 (92.1%), 282 (89.5%), and 259 (82.2%) patients, respectively. Primary patency rates at 6, 12, and 24 months were 39.5%, 34.8%, and 27.2% for RC_AVF, 58.3%, 44.4%, and 27.8% for BC_AVF, and 40.0%, 42.1%, and 22.2% for BB_AVF (p = 0.15). Secondary patency rates at 6, 12, and 24 months were 65.7%, 63.8%, and 59.0% for RC_AVF, 77.7%, 72.0%, and 59.6% for BC_AVF, and 65.0%, 68.4%, and 61.1% for BB_AVF (p = 0.29). Factors associated with lower primary and secondary patency were hemodialysis at time of arteriovenous fistula formation (p = 0.037 and p = 0.024, respectively) and higher Charlson Comorbidity Index (p = 0.036 and p < 0.001, respectively). Previous kidney transplant showed inferior primary patency (p = 0.005); higher age inferior secondary patency (p < 0.001).
Discussion
Vascular access care remains challenging and salvage interventions are often needed to achieve maturation or maintain patency. Strict adherence to standardized outcome reporting in vascular access surgery paints a more realistic picture of arteriovenous fistula patency and enables reliable intercenter comparison.

 求助内容:
求助内容: 应助结果提醒方式:
应助结果提醒方式:


