Acute myocarditis after administration of BNT162b2 vaccine against COVID-19.
IF 0.7
Q4 CARDIAC & CARDIOVASCULAR SYSTEMS
引用次数: 0
Abstract
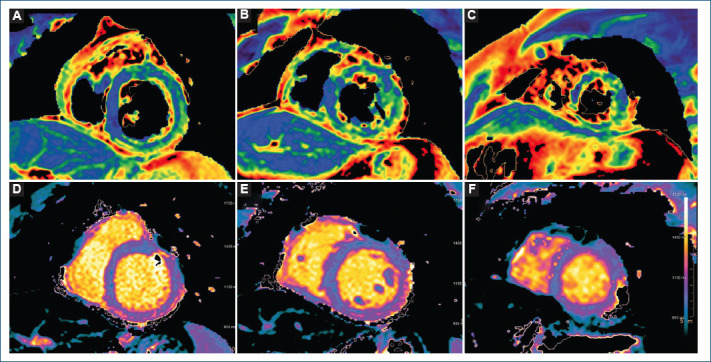
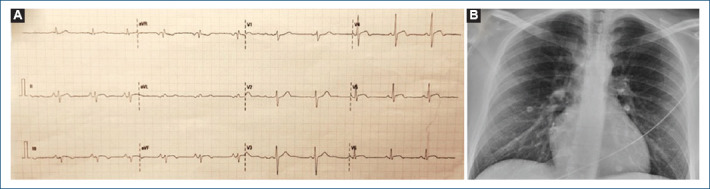
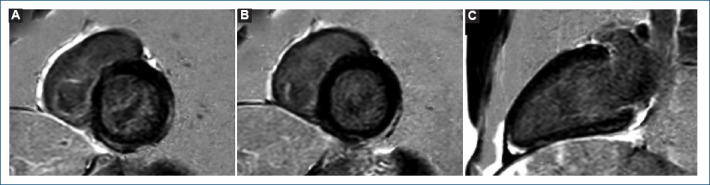
*Correspondence: Juan F. Cueva-Recalde E-mail: franciscocueva@hotmail.com Available online: 04-04-2023 Arch Cardiol Mex. 2023;93(2):243-245 www.archivoscardiologia.com Date of reception: 23-08-2021 Date of acceptance: 17-02-2022 DOI: 10.24875/ACM.21000270 COVID-19 mRNA vaccines have been associated with the development of myocarditis, specifically in young men after the administration of the second dose, with a low rate of 1 case/10 000 vaccinated people1. We present the case of a 28-year-old male patient without the previous medical history referring chest pain episodes for the past 3 days. He received the second dose of BNT162b2 vaccine against COVID-19 4 days before. Electrocardiogram showed 1mm ST-segment elevation in lateral and inferior leads (Fig. 1) and high-sensitivity cardiac troponin T (hs-cTnT)) was 1470 ng/L (< 14 ng/L). Normal left ventricle (LV) ejection fraction without wall motion abnormalities (WMA) was noted in echocardiogram. Acute COVID-19 infection was ruled out by negative SARS-CoV-2 polymerase chain reaction test, chest X-ray was normal (Fig. 1). The patient was admitted and remained asymptomatic requiring no treatment. The peak value of hs-cTnT (2200 ng/L) was reached the day 5 after vaccination. Given its low yield, no serological tests for cardiotrophic viruses were ordered. Within the first 24 h, cardiac magnetic resonance imaging was performed, and mapping sequences showed increased T2 values in inferior
新冠病毒BNT162b2疫苗接种后急性心肌炎。
本文章由计算机程序翻译,如有差异,请以英文原文为准。
求助全文
约1分钟内获得全文
求助全文
来源期刊

Archivos de cardiologia de Mexico
Medicine-Cardiology and Cardiovascular Medicine
CiteScore
0.80
自引率
20.00%
发文量
176
审稿时长
18 weeks
 求助内容:
求助内容: 应助结果提醒方式:
应助结果提醒方式:


