{"title":"A nomogram based on clinical factors to predict calendar year readmission in patients with ulcerative colitis.","authors":"Ying Xiang, Ying Yuan, Jinyan Liu, Xinwen Xu, Zhenyu Wang, Shahzeb Hassan, Yue Wu, Qi Sun, Yonghua Shen, Lei Wang, Hua Yang, Jing Sun, Guifang Xu, Qin Huang","doi":"10.1177/17562848231189124","DOIUrl":null,"url":null,"abstract":"<p><strong>Background: </strong>Readmission shortly after discharge is indicative of an increased disease severity for patients with ulcerative colitis (UC) and ineffectiveness to medical therapy, which may contribute to a dismal prognosis.</p><p><strong>Objectives: </strong>This study aimed to explore prognostic variables with a nomogram to predict unplanned UC-related readmission within 1 year after discharge.</p><p><strong>Design: </strong>A retrospective cohort study.</p><p><strong>Methods: </strong>Electronic medical records of all UC patients treated at our center between 1 January 2014 and 31 June 2021 were reviewed. A comprehensive analysis of various characteristics, such as demographics, comorbidities, medical history, follow-up appointments, admission endoscopy, histopathologic features, etc., was used to determine the primary end point, which was unplanned UC-related calendar year readmission.</p><p><strong>Results: </strong>We found that the unplanned UC-related readmission rate within 1 year was 20.8%. In multivariable cox analysis, the predictors of the Elixhauser comorbidity index [Hazard ratio (HR): 3.50, 95% confidence interval (CI): 1.93-6.37], regular follow-up (HR: 0.29, 95% CI: 0.16-0.53), any history of corticosteroid use (HR: 3.38, 95% CI: 1.83-6.27), seral level of C-reactive protein (HR: 1.01, 95% CI: 1.00-1.02), and the UC endoscopic index of severity (HR: 1.29, 95% CI: 1.05-1.57) independently predicted calendar year readmission after discharge. The established nomogram had a consistently high accuracy in predicting calendar year readmission in the training cohort, with a concordance index of 0.784, 0.825, and 0.837 at 13, 26, and 52 weeks, respectively, which was validated in both the internal and external validation cohorts. Therefore, UC patients were divided into clinically low-, high-, and extremely high-risk groups for readmission, based on the calculated score of 272.5 and 378.</p><p><strong>Conclusion: </strong>The established nomogram showed good discrimination and calibration powers in predicting calendar year readmission in high-risk UC patients, who may need intensive treatment and regular outpatient visits.</p>","PeriodicalId":23022,"journal":{"name":"Therapeutic Advances in Gastroenterology","volume":"16 ","pages":"17562848231189124"},"PeriodicalIF":3.4000,"publicationDate":"2023-01-01","publicationTypes":"Journal Article","fieldsOfStudy":null,"isOpenAccess":false,"openAccessPdf":"https://ftp.ncbi.nlm.nih.gov/pub/pmc/oa_pdf/4f/96/10.1177_17562848231189124.PMC10392194.pdf","citationCount":"0","resultStr":null,"platform":"Semanticscholar","paperid":null,"PeriodicalName":"Therapeutic Advances in Gastroenterology","FirstCategoryId":"3","ListUrlMain":"https://doi.org/10.1177/17562848231189124","RegionNum":3,"RegionCategory":"医学","ArticlePicture":[],"TitleCN":null,"AbstractTextCN":null,"PMCID":null,"EPubDate":"","PubModel":"","JCR":"","JCRName":"","Score":null,"Total":0}
引用次数: 0
Abstract
Background: Readmission shortly after discharge is indicative of an increased disease severity for patients with ulcerative colitis (UC) and ineffectiveness to medical therapy, which may contribute to a dismal prognosis.
Objectives: This study aimed to explore prognostic variables with a nomogram to predict unplanned UC-related readmission within 1 year after discharge.
Design: A retrospective cohort study.
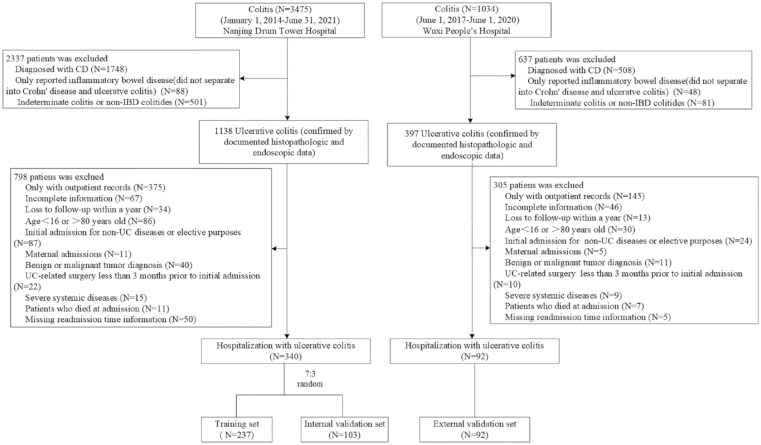
Methods: Electronic medical records of all UC patients treated at our center between 1 January 2014 and 31 June 2021 were reviewed. A comprehensive analysis of various characteristics, such as demographics, comorbidities, medical history, follow-up appointments, admission endoscopy, histopathologic features, etc., was used to determine the primary end point, which was unplanned UC-related calendar year readmission.
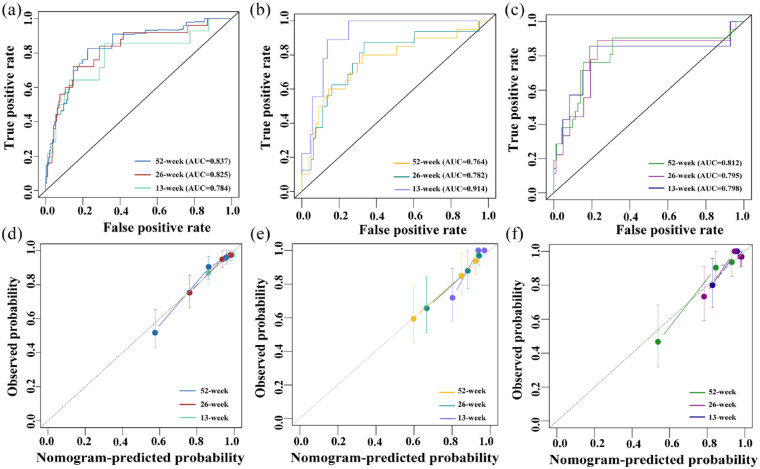
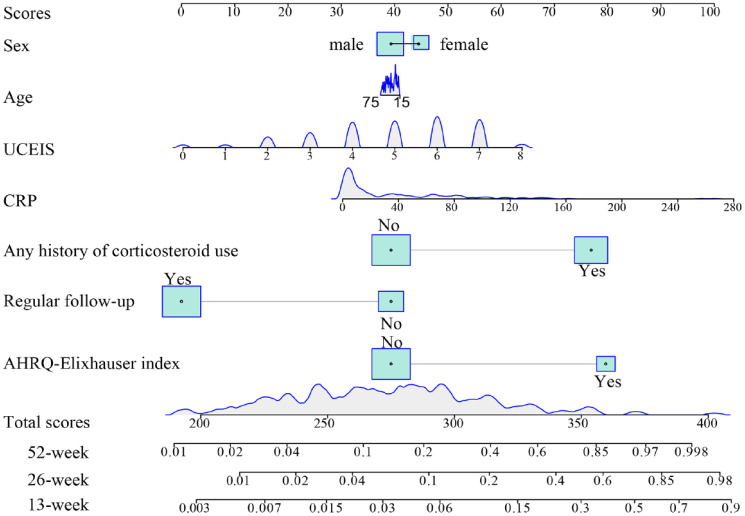
Results: We found that the unplanned UC-related readmission rate within 1 year was 20.8%. In multivariable cox analysis, the predictors of the Elixhauser comorbidity index [Hazard ratio (HR): 3.50, 95% confidence interval (CI): 1.93-6.37], regular follow-up (HR: 0.29, 95% CI: 0.16-0.53), any history of corticosteroid use (HR: 3.38, 95% CI: 1.83-6.27), seral level of C-reactive protein (HR: 1.01, 95% CI: 1.00-1.02), and the UC endoscopic index of severity (HR: 1.29, 95% CI: 1.05-1.57) independently predicted calendar year readmission after discharge. The established nomogram had a consistently high accuracy in predicting calendar year readmission in the training cohort, with a concordance index of 0.784, 0.825, and 0.837 at 13, 26, and 52 weeks, respectively, which was validated in both the internal and external validation cohorts. Therefore, UC patients were divided into clinically low-, high-, and extremely high-risk groups for readmission, based on the calculated score of 272.5 and 378.
Conclusion: The established nomogram showed good discrimination and calibration powers in predicting calendar year readmission in high-risk UC patients, who may need intensive treatment and regular outpatient visits.
期刊介绍:
Therapeutic Advances in Gastroenterology is an open access journal which delivers the highest quality peer-reviewed original research articles, reviews, and scholarly comment on pioneering efforts and innovative studies in the medical treatment of gastrointestinal and hepatic disorders. The journal has a strong clinical and pharmacological focus and is aimed at an international audience of clinicians and researchers in gastroenterology and related disciplines, providing an online forum for rapid dissemination of recent research and perspectives in this area.
The editors welcome original research articles across all areas of gastroenterology and hepatology.
The journal publishes original research articles and review articles primarily. Original research manuscripts may include laboratory, animal or human/clinical studies – all phases. Letters to the Editor and Case Reports will also be considered.

 求助内容:
求助内容: 应助结果提醒方式:
应助结果提醒方式:


