Online Self-Triage of Ear or Hearing Concerns in a Patient Portal: Comparison of Subsequent Diagnoses and Hospitalizations to National Emergency Department and National Ambulatory Ear or Hearing Visits.
Frederick North, Teresa B Jensen, Jennifer Pecina, Nathaniel E Miller, Michelle Duvall, Elissa M Nelson, Matthew C Thompson, Brenda J Johnson, Brian A Crum, Robert Stroebel
{"title":"Online Self-Triage of Ear or Hearing Concerns in a Patient Portal: Comparison of Subsequent Diagnoses and Hospitalizations to National Emergency Department and National Ambulatory Ear or Hearing Visits.","authors":"Frederick North, Teresa B Jensen, Jennifer Pecina, Nathaniel E Miller, Michelle Duvall, Elissa M Nelson, Matthew C Thompson, Brenda J Johnson, Brian A Crum, Robert Stroebel","doi":"10.1177/23333928231186209","DOIUrl":null,"url":null,"abstract":"<p><strong>Background: </strong>Although online self-triage is easily accessible, little is known about the patients who use self-triage or their subsequent diagnoses. We compared ear/hearing self-triage subsequent diagnoses to ear/hearing visit diagnoses in emergency departments (ED) and ambulatory clinics across the United States.</p><p><strong>Methods: </strong>We compared International Classification of Diseases version 10 (ICD10) coded diagnoses following online self-triage for ear/hearing concerns with those from national ED and ambulatory clinic samples. We used data from the Centers for Disease Control (CDC) National Hospital Ambulatory Medical Care Survey (NHAMCS) and National Ambulatory Medical Care Survey (NAMCS) for comparison. Using matched ear/hearing diagnostic categories for those aged 1 and over, we compared self-triage diagnosis frequencies with national ED and ambulatory diagnosis frequencies.</p><p><strong>Results: </strong>Following ear/hearing self-triage, there were 1092 subsequent office visits with a primary diagnosis code. For five frequently diagnosed ear/hearing conditions (i.e., suppurative and nonsuppurative otitis media [OM], otalgia, otitis externa, and cerumen impaction), there was a strong correlation between diagnosis counts made following self-triage and estimated counts of national ED visit diagnoses (r = 0.94; CI 95% [0.37 to 0.99]; <i>p </i>= .016, adjusted r<sup>2</sup> = 0.85). Seven diagnoses were available to compare with the national ambulatory sample; correlation was r = 0.79; CI 95% [0.08 to 0.97]; <i>p </i>= .037, adjusted r<sup>2 </sup>= 0.54. For ages 1 and over, estimated hospital admissions from the national ED visits for ear/hearing were 0.76%, CI 95% [0.28-2.1%]; estimated total national ear/hearing ED visits were 7.5 million (for 4 years, 2016 through 2019).</p><p><strong>Conclusion: </strong>The strong correlation of ear-related self-triage diagnoses with national ED diagnoses and the low hospitalization risk for these diagnoses suggests that there is an opportunity for self-triage of ear/hearing concerns to decrease ED visits for these symptoms.</p>","PeriodicalId":12951,"journal":{"name":"Health Services Research and Managerial Epidemiology","volume":"10 ","pages":"23333928231186209"},"PeriodicalIF":1.5000,"publicationDate":"2023-01-01","publicationTypes":"Journal Article","fieldsOfStudy":null,"isOpenAccess":false,"openAccessPdf":"https://ftp.ncbi.nlm.nih.gov/pub/pmc/oa_pdf/d3/52/10.1177_23333928231186209.PMC10387706.pdf","citationCount":"1","resultStr":null,"platform":"Semanticscholar","paperid":null,"PeriodicalName":"Health Services Research and Managerial Epidemiology","FirstCategoryId":"1085","ListUrlMain":"https://doi.org/10.1177/23333928231186209","RegionNum":0,"RegionCategory":null,"ArticlePicture":[],"TitleCN":null,"AbstractTextCN":null,"PMCID":null,"EPubDate":"","PubModel":"","JCR":"Q3","JCRName":"HEALTH POLICY & SERVICES","Score":null,"Total":0}
引用次数: 1
Abstract
Background: Although online self-triage is easily accessible, little is known about the patients who use self-triage or their subsequent diagnoses. We compared ear/hearing self-triage subsequent diagnoses to ear/hearing visit diagnoses in emergency departments (ED) and ambulatory clinics across the United States.
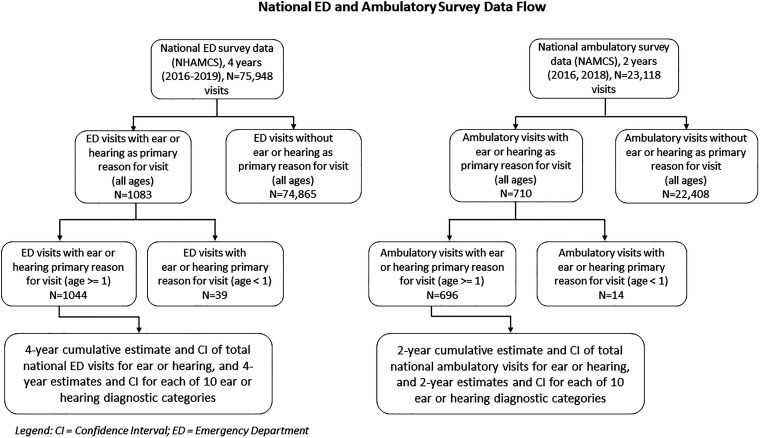
Methods: We compared International Classification of Diseases version 10 (ICD10) coded diagnoses following online self-triage for ear/hearing concerns with those from national ED and ambulatory clinic samples. We used data from the Centers for Disease Control (CDC) National Hospital Ambulatory Medical Care Survey (NHAMCS) and National Ambulatory Medical Care Survey (NAMCS) for comparison. Using matched ear/hearing diagnostic categories for those aged 1 and over, we compared self-triage diagnosis frequencies with national ED and ambulatory diagnosis frequencies.
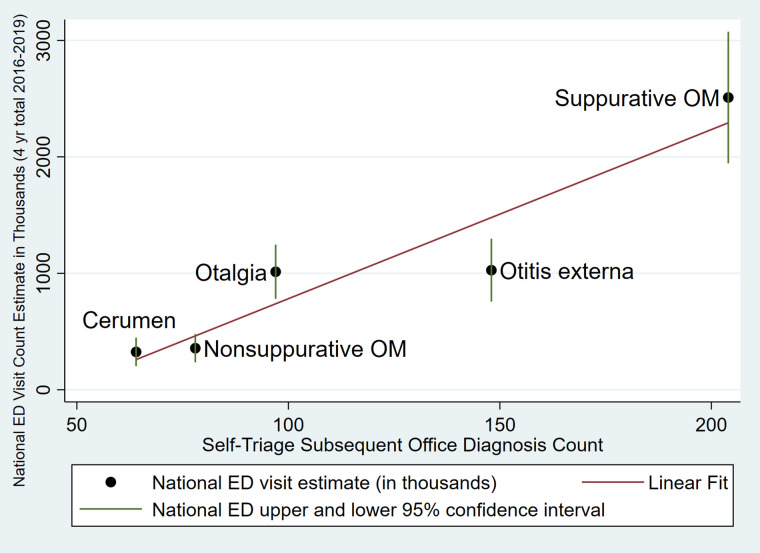
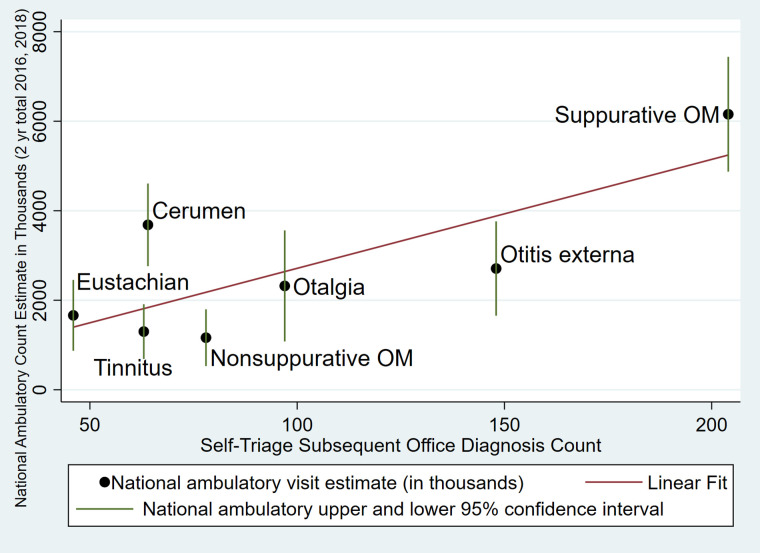
Results: Following ear/hearing self-triage, there were 1092 subsequent office visits with a primary diagnosis code. For five frequently diagnosed ear/hearing conditions (i.e., suppurative and nonsuppurative otitis media [OM], otalgia, otitis externa, and cerumen impaction), there was a strong correlation between diagnosis counts made following self-triage and estimated counts of national ED visit diagnoses (r = 0.94; CI 95% [0.37 to 0.99]; p = .016, adjusted r2 = 0.85). Seven diagnoses were available to compare with the national ambulatory sample; correlation was r = 0.79; CI 95% [0.08 to 0.97]; p = .037, adjusted r2 = 0.54. For ages 1 and over, estimated hospital admissions from the national ED visits for ear/hearing were 0.76%, CI 95% [0.28-2.1%]; estimated total national ear/hearing ED visits were 7.5 million (for 4 years, 2016 through 2019).
Conclusion: The strong correlation of ear-related self-triage diagnoses with national ED diagnoses and the low hospitalization risk for these diagnoses suggests that there is an opportunity for self-triage of ear/hearing concerns to decrease ED visits for these symptoms.

 求助内容:
求助内容: 应助结果提醒方式:
应助结果提醒方式:


