{"title":"Cost-Effectiveness of Humidified High-Flow Therapy (HHFT) for COPD Patients on Long-Term Oxygen Therapy.","authors":"Erik J Groessl, Steven R Tally, Naomi Hillery","doi":"10.2147/CEOR.S400739","DOIUrl":null,"url":null,"abstract":"<p><strong>Purpose: </strong>Chronic obstructive pulmonary disease (COPD) is the third leading cause of mortality, and is associated with significant respiratory impairment, decreased quality of life, and high health care costs. Recent evidence indicates significant clinical benefit results from adding humidified high-flow therapy (HHFT) to standard long-term oxygen therapy (LTOT) as a home-based therapy in persons with severe COPD. The objective was to evaluate the cost-effectiveness of adding HHFT to standard treatment of COPD patients using LTOT with US healthcare cost estimates.</p><p><strong>Patients and methods: </strong>A Markov state-transition model was developed using data from a prospective clinical trial of adding HHFT to standard therapy for persons with severe COPD using LTOT. The analysis was conducted from the US health care system perspective using a 5-year time horizon and 3% discount rate. QALYs and downstream healthcare costs were modeled. One-way and probabilistic sensitivity analyses were used to examine the impact of input parameters on the incremental net monetary benefit (NMB).</p><p><strong>Results: </strong>Incremental QALYs accrued were 0.058 (2.047 vs 1.989 QALYs for HHFT and standard therapy groups respectively). Incremental total costs were -$3939 ($47,516 vs $51,455 for HHFT and standard therapy groups respectively). Thus, HHFT was the dominant treatment in the analysis, resulting on both better health and lower total costs. Varying utility and cost inputs individually never resulted in NMB approaching 0. Probabilistic analyses indicate that HHFT is cost-effective in 84% of simulations.</p><p><strong>Conclusion: </strong>Our results indicate that the reductions in acute exacerbations of COPD (AECOPDs) that result from adding HHFT for persons with COPD on LTOT will produce both health benefit (QALYs) and cost savings. Cost savings occur because the HHFT device costs are more than offset by reductions in costly COPD exacerbations. Health care systems and payors can benefit from wider implementation of HHFT with existing treatments.</p>","PeriodicalId":47313,"journal":{"name":"ClinicoEconomics and Outcomes Research","volume":"15 ","pages":"239-250"},"PeriodicalIF":2.1000,"publicationDate":"2023-01-01","publicationTypes":"Journal Article","fieldsOfStudy":null,"isOpenAccess":false,"openAccessPdf":"https://ftp.ncbi.nlm.nih.gov/pub/pmc/oa_pdf/ef/72/ceor-15-239.PMC10083032.pdf","citationCount":"1","resultStr":null,"platform":"Semanticscholar","paperid":null,"PeriodicalName":"ClinicoEconomics and Outcomes Research","FirstCategoryId":"1085","ListUrlMain":"https://doi.org/10.2147/CEOR.S400739","RegionNum":0,"RegionCategory":null,"ArticlePicture":[],"TitleCN":null,"AbstractTextCN":null,"PMCID":null,"EPubDate":"","PubModel":"","JCR":"Q3","JCRName":"HEALTH CARE SCIENCES & SERVICES","Score":null,"Total":0}
引用次数: 1
Abstract
Purpose: Chronic obstructive pulmonary disease (COPD) is the third leading cause of mortality, and is associated with significant respiratory impairment, decreased quality of life, and high health care costs. Recent evidence indicates significant clinical benefit results from adding humidified high-flow therapy (HHFT) to standard long-term oxygen therapy (LTOT) as a home-based therapy in persons with severe COPD. The objective was to evaluate the cost-effectiveness of adding HHFT to standard treatment of COPD patients using LTOT with US healthcare cost estimates.
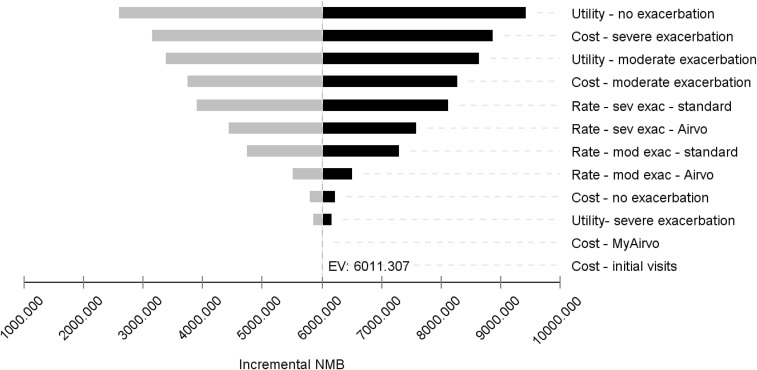
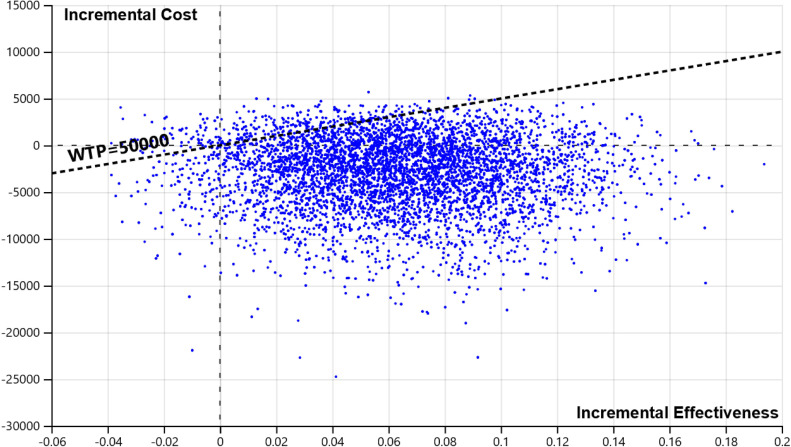
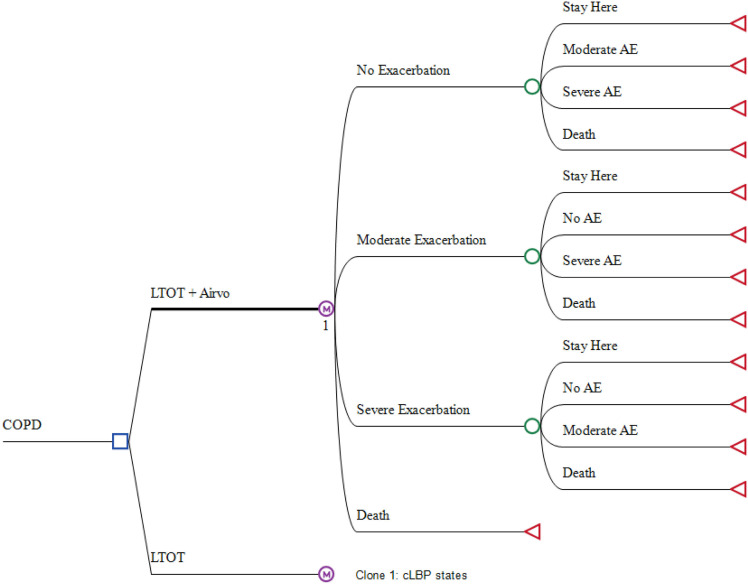
Patients and methods: A Markov state-transition model was developed using data from a prospective clinical trial of adding HHFT to standard therapy for persons with severe COPD using LTOT. The analysis was conducted from the US health care system perspective using a 5-year time horizon and 3% discount rate. QALYs and downstream healthcare costs were modeled. One-way and probabilistic sensitivity analyses were used to examine the impact of input parameters on the incremental net monetary benefit (NMB).
Results: Incremental QALYs accrued were 0.058 (2.047 vs 1.989 QALYs for HHFT and standard therapy groups respectively). Incremental total costs were -$3939 ($47,516 vs $51,455 for HHFT and standard therapy groups respectively). Thus, HHFT was the dominant treatment in the analysis, resulting on both better health and lower total costs. Varying utility and cost inputs individually never resulted in NMB approaching 0. Probabilistic analyses indicate that HHFT is cost-effective in 84% of simulations.
Conclusion: Our results indicate that the reductions in acute exacerbations of COPD (AECOPDs) that result from adding HHFT for persons with COPD on LTOT will produce both health benefit (QALYs) and cost savings. Cost savings occur because the HHFT device costs are more than offset by reductions in costly COPD exacerbations. Health care systems and payors can benefit from wider implementation of HHFT with existing treatments.

 求助内容:
求助内容: 应助结果提醒方式:
应助结果提醒方式:


