A fatal case report of invasive pulmonary aspergillosis and mucormycosis coinfection in an immunocompetent patient with coronavirus disease 2019 in Korea.
Jin Hyoung Kim, Misung Kim, Soyeoun Lim, Sun Young Park, Yangjin Jegal, Taehoon Lee, Byung Ju Kang
{"title":"A fatal case report of invasive pulmonary aspergillosis and mucormycosis coinfection in an immunocompetent patient with coronavirus disease 2019 in Korea.","authors":"Jin Hyoung Kim, Misung Kim, Soyeoun Lim, Sun Young Park, Yangjin Jegal, Taehoon Lee, Byung Ju Kang","doi":"10.4266/acc.2021.01340","DOIUrl":null,"url":null,"abstract":"<p><p>Systemic glucocorticoid treatment is highly recommended in critically ill coronavirus disease 2019 (COVID-19) patients. However, secondary fungal infections are of concern in such patients. Here, we describe the first case of COVID-19-associated invasive pulmonary aspergillosis (CAPA) and COVID-19-associated mucormycosis (CAM) coinfection in a COVID-19 positive immunocompetent patient in Korea. A 69-year-old man was admitted to our hospital with COVID-19 pneumonia. He had no underlying comorbidities and was not taking medications. He received remdesivir, dexamethasone, and antibiotic therapy under mechanical ventilation. Although his condition improved temporarily, multiple cavities were observed on chest computed tomography, and Aspergillus fumigatus was cultured from tracheal aspiration culture. He was diagnosed with probable CAPA and received voriconazole therapy. However, his condition was not significantly improved despite having received voriconazole therapy for 4 weeks. After release from COVID-19 quarantine, he underwent bronchoscopy examination and was then finally diagnosed with CAPA and CAM coinfection on bronchoscopic biopsy. Antifungal treatment was changed to liposomal amphotericin B. However, his progress deteriorated, and he died 4 months after admission. This case highlights that clinical suspicion and active checkups are required to diagnose secondary fungal infections in immunocompetent COVID-19 patients who receive concurrent glucocorticoid therapy.</p>","PeriodicalId":44118,"journal":{"name":"Acute and Critical Care","volume":null,"pages":null},"PeriodicalIF":1.7000,"publicationDate":"2023-08-01","publicationTypes":"Journal Article","fieldsOfStudy":null,"isOpenAccess":false,"openAccessPdf":"https://ftp.ncbi.nlm.nih.gov/pub/pmc/oa_pdf/14/4c/acc-2021-01340.PMC10497891.pdf","citationCount":"2","resultStr":null,"platform":"Semanticscholar","paperid":null,"PeriodicalName":"Acute and Critical Care","FirstCategoryId":"1085","ListUrlMain":"https://doi.org/10.4266/acc.2021.01340","RegionNum":0,"RegionCategory":null,"ArticlePicture":[],"TitleCN":null,"AbstractTextCN":null,"PMCID":null,"EPubDate":"","PubModel":"","JCR":"Q3","JCRName":"CRITICAL CARE MEDICINE","Score":null,"Total":0}
引用次数: 2
Abstract
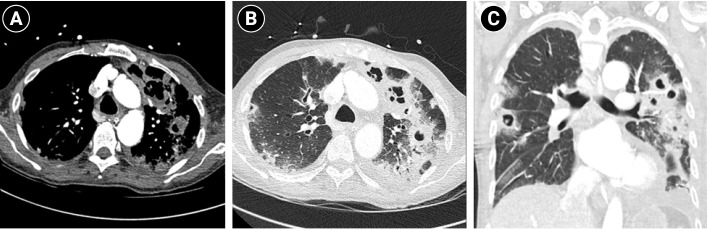
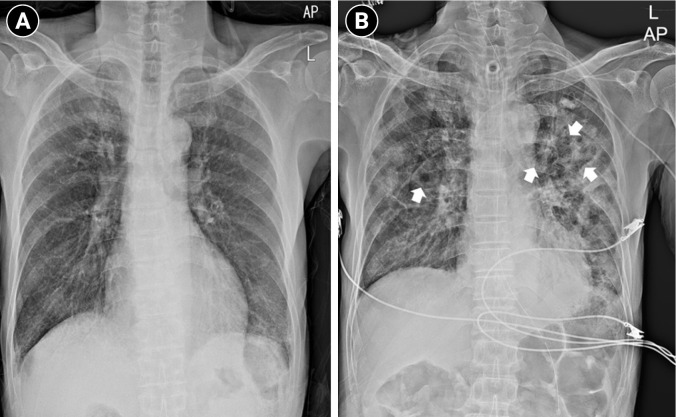
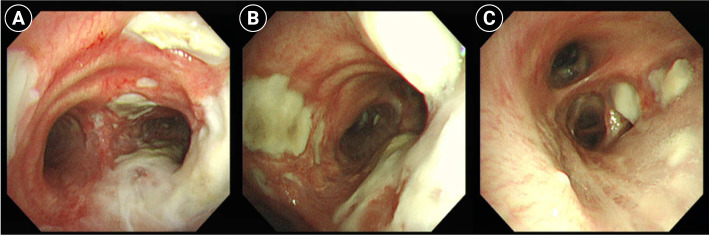
Systemic glucocorticoid treatment is highly recommended in critically ill coronavirus disease 2019 (COVID-19) patients. However, secondary fungal infections are of concern in such patients. Here, we describe the first case of COVID-19-associated invasive pulmonary aspergillosis (CAPA) and COVID-19-associated mucormycosis (CAM) coinfection in a COVID-19 positive immunocompetent patient in Korea. A 69-year-old man was admitted to our hospital with COVID-19 pneumonia. He had no underlying comorbidities and was not taking medications. He received remdesivir, dexamethasone, and antibiotic therapy under mechanical ventilation. Although his condition improved temporarily, multiple cavities were observed on chest computed tomography, and Aspergillus fumigatus was cultured from tracheal aspiration culture. He was diagnosed with probable CAPA and received voriconazole therapy. However, his condition was not significantly improved despite having received voriconazole therapy for 4 weeks. After release from COVID-19 quarantine, he underwent bronchoscopy examination and was then finally diagnosed with CAPA and CAM coinfection on bronchoscopic biopsy. Antifungal treatment was changed to liposomal amphotericin B. However, his progress deteriorated, and he died 4 months after admission. This case highlights that clinical suspicion and active checkups are required to diagnose secondary fungal infections in immunocompetent COVID-19 patients who receive concurrent glucocorticoid therapy.

 求助内容:
求助内容: 应助结果提醒方式:
应助结果提醒方式:


