Vincenzo Accurso, Marco Santoro, Salvatrice Mancuso, Mariasanta Napolitano, Melania Carlisi, Marta Mattana, Chiara Russo, Alessandro Di Stefano, Davide Sirocchi, Sergio Siragusa
{"title":"The Essential Thrombocythemia in 2020: What We Know and Where We Still Have to Dig Deep.","authors":"Vincenzo Accurso, Marco Santoro, Salvatrice Mancuso, Mariasanta Napolitano, Melania Carlisi, Marta Mattana, Chiara Russo, Alessandro Di Stefano, Davide Sirocchi, Sergio Siragusa","doi":"10.1177/2634853520978210","DOIUrl":null,"url":null,"abstract":"<p><p>The Essential Thrombocythemia is a Chronic Philadelphia-negative Myeloproliferative Neoplasm characterized by a survival curve that is only slightly worse than that of age- and sex-adjusted healthy population. The criteria for diagnosis were reviewed in 2016 by WHO. The incidence varies from 0.2 to 2.5:100 000 people per year, with a prevalence of 38 to 57 cases per 100 000 people. The main characteristics of ET are the marked thrombocytosis and the high frequency of thrombosis. The spectrum of symptoms is quite wide, but fatigue results to be the most frequent. Thrombosis is frequently observed, often occurring before or at the time of diagnosis. The classification of thrombotic risk has undergone several revisions. Recently, the revised-IPSET-t has distinguished 4 risk classes, from very low risk to high risk. Driver mutations seem to influence thrombotic risk and prognosis, while the role of sub-driver mutations still remains uncertain. Antiplatelet therapy is recommended in all patients aged ⩾ 60 years and in those with a positive history of thrombosis or with cardiovascular risk factors, while cytoreductive therapy with hydroxyurea or interferon is reserved for high-risk patients.</p>","PeriodicalId":43083,"journal":{"name":"Clinical Medicine Insights-Blood Disorders","volume":"13 ","pages":"2634853520978210"},"PeriodicalIF":3.0000,"publicationDate":"2020-01-01","publicationTypes":"Journal Article","fieldsOfStudy":null,"isOpenAccess":false,"openAccessPdf":"https://sci-hub-pdf.com/10.1177/2634853520978210","citationCount":"22","resultStr":null,"platform":"Semanticscholar","paperid":null,"PeriodicalName":"Clinical Medicine Insights-Blood Disorders","FirstCategoryId":"1085","ListUrlMain":"https://doi.org/10.1177/2634853520978210","RegionNum":0,"RegionCategory":null,"ArticlePicture":[],"TitleCN":null,"AbstractTextCN":null,"PMCID":null,"EPubDate":"","PubModel":"","JCR":"Q2","JCRName":"Medicine","Score":null,"Total":0}
引用次数: 22
Abstract
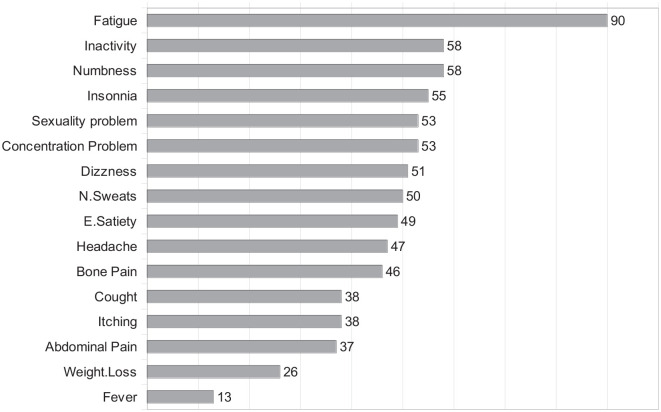
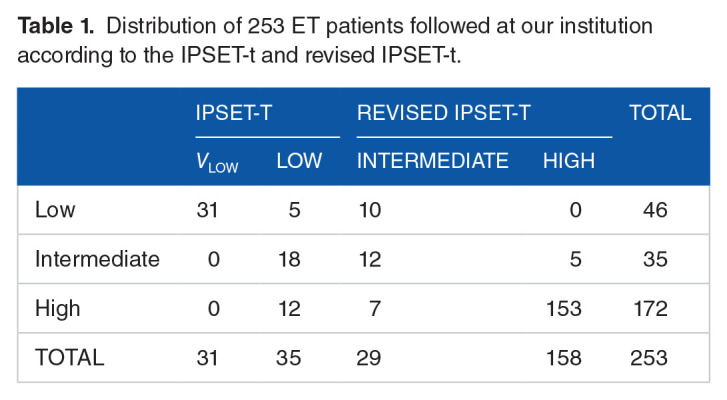
The Essential Thrombocythemia is a Chronic Philadelphia-negative Myeloproliferative Neoplasm characterized by a survival curve that is only slightly worse than that of age- and sex-adjusted healthy population. The criteria for diagnosis were reviewed in 2016 by WHO. The incidence varies from 0.2 to 2.5:100 000 people per year, with a prevalence of 38 to 57 cases per 100 000 people. The main characteristics of ET are the marked thrombocytosis and the high frequency of thrombosis. The spectrum of symptoms is quite wide, but fatigue results to be the most frequent. Thrombosis is frequently observed, often occurring before or at the time of diagnosis. The classification of thrombotic risk has undergone several revisions. Recently, the revised-IPSET-t has distinguished 4 risk classes, from very low risk to high risk. Driver mutations seem to influence thrombotic risk and prognosis, while the role of sub-driver mutations still remains uncertain. Antiplatelet therapy is recommended in all patients aged ⩾ 60 years and in those with a positive history of thrombosis or with cardiovascular risk factors, while cytoreductive therapy with hydroxyurea or interferon is reserved for high-risk patients.


 求助内容:
求助内容: 应助结果提醒方式:
应助结果提醒方式:


