David Singer, Philippe Thompson-Leduc, Deepshekhar Gupta, Sara Poston, Wendy Y Cheng, Siyu Ma, John E Pawlowski, Mei Sheng Duh, Francesca Devine, Azeem Banatwala, Emma Bernstein, Francis A Farraye
{"title":"Economic and Clinical Burden of Herpes Zoster Among Patients With Inflammatory Bowel Disease in the United States.","authors":"David Singer, Philippe Thompson-Leduc, Deepshekhar Gupta, Sara Poston, Wendy Y Cheng, Siyu Ma, John E Pawlowski, Mei Sheng Duh, Francesca Devine, Azeem Banatwala, Emma Bernstein, Francis A Farraye","doi":"10.1093/crocol/otad033","DOIUrl":null,"url":null,"abstract":"<p><strong>Background: </strong>Patients with ulcerative colitis (UC) or Crohn's disease (CD) are at increased risk of herpes zoster (HZ); however, relevant cost and healthcare resource utilization (HCRU) data are limited.</p><p><strong>Methods: </strong>We estimated HCRU (hospitalization, emergency department [ED], and outpatient visits) and costs in patients with UC or CD, with and without HZ, using administrative claims data (October 2015-February 2020). HCRU and costs (2020 US dollars) were compared at 1 month, 1 quarter, and 1 year after the index date, using propensity score adjustment and generalized linear models.</p><p><strong>Results: </strong>In total, 20 948 patients were included: UC+/HZ+ (<i>n</i> = 431), UC+/HZ- (<i>n</i> = 10 285), CD+/HZ+ (<i>n</i> = 435), and CD+/HZ- (<i>n</i> = 9797). Patients with HZ had higher all-cause HCRU rates and all-cause total healthcare costs relative to those without HZ. In the first month, adjusted incidence rate ratios (aIRRs) for hospitalizations and ED visits for patients with UC and HZ compared with UC alone were 2.87 (95% confidence interval [CI], 1.93-4.27) and 2.66 (95% CI,1.74-4.05), respectively; for those with CD and HZ, aIRRs were 3.34 (95% CI, 2.38-4.70) and 3.31 (95% CI, 2.32-4.71), respectively, compared with CD alone (all <i>P</i> < .001). Adjusted cost differences in UC and CD cohorts with HZ over the first month were $2189 and $3774, respectively, chiefly driven by higher inpatient costs. The incremental impact on HCRU and costs in cohorts with HZ predominantly occurred during the first quarter following diagnosis.</p><p><strong>Conclusions: </strong>HZ is associated with increased HCRU and costs in patients with UC and CD, especially shortly after diagnosis.</p>","PeriodicalId":10847,"journal":{"name":"Crohn's & Colitis 360","volume":"5 3","pages":"otad033"},"PeriodicalIF":1.8000,"publicationDate":"2023-07-01","publicationTypes":"Journal Article","fieldsOfStudy":null,"isOpenAccess":false,"openAccessPdf":"https://www.ncbi.nlm.nih.gov/pmc/articles/PMC10368335/pdf/","citationCount":"0","resultStr":null,"platform":"Semanticscholar","paperid":null,"PeriodicalName":"Crohn's & Colitis 360","FirstCategoryId":"1085","ListUrlMain":"https://doi.org/10.1093/crocol/otad033","RegionNum":0,"RegionCategory":null,"ArticlePicture":[],"TitleCN":null,"AbstractTextCN":null,"PMCID":null,"EPubDate":"","PubModel":"","JCR":"Q3","JCRName":"GASTROENTEROLOGY & HEPATOLOGY","Score":null,"Total":0}
引用次数: 0
Abstract
Background: Patients with ulcerative colitis (UC) or Crohn's disease (CD) are at increased risk of herpes zoster (HZ); however, relevant cost and healthcare resource utilization (HCRU) data are limited.
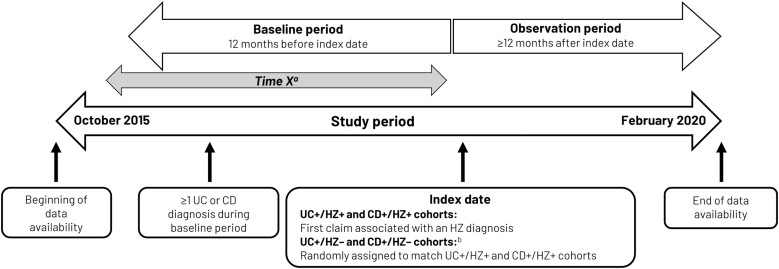
Methods: We estimated HCRU (hospitalization, emergency department [ED], and outpatient visits) and costs in patients with UC or CD, with and without HZ, using administrative claims data (October 2015-February 2020). HCRU and costs (2020 US dollars) were compared at 1 month, 1 quarter, and 1 year after the index date, using propensity score adjustment and generalized linear models.
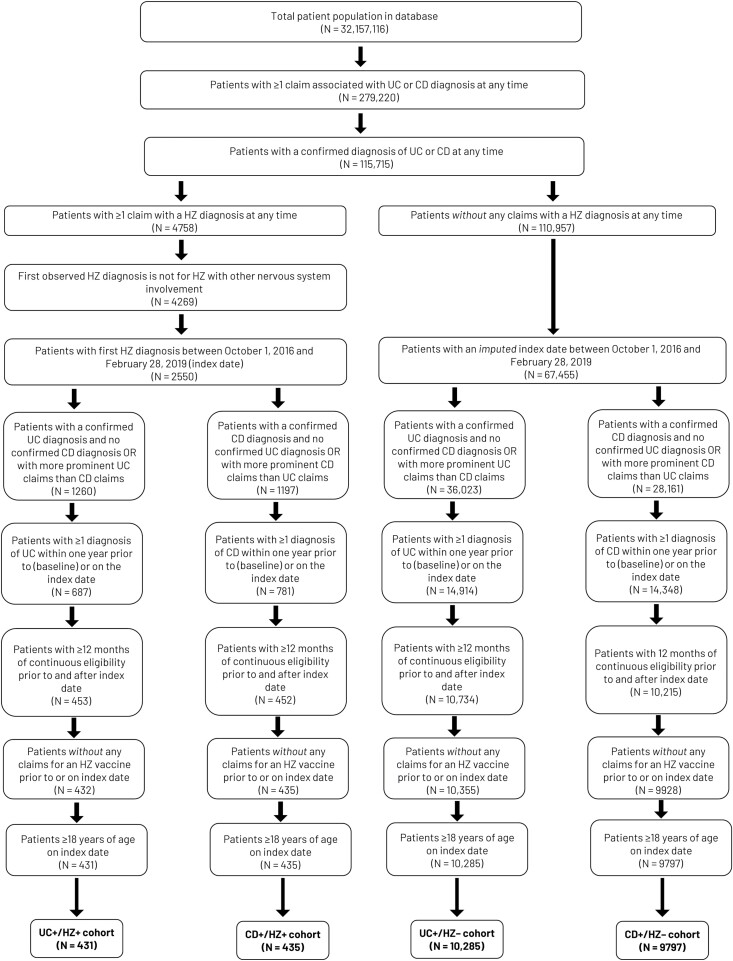
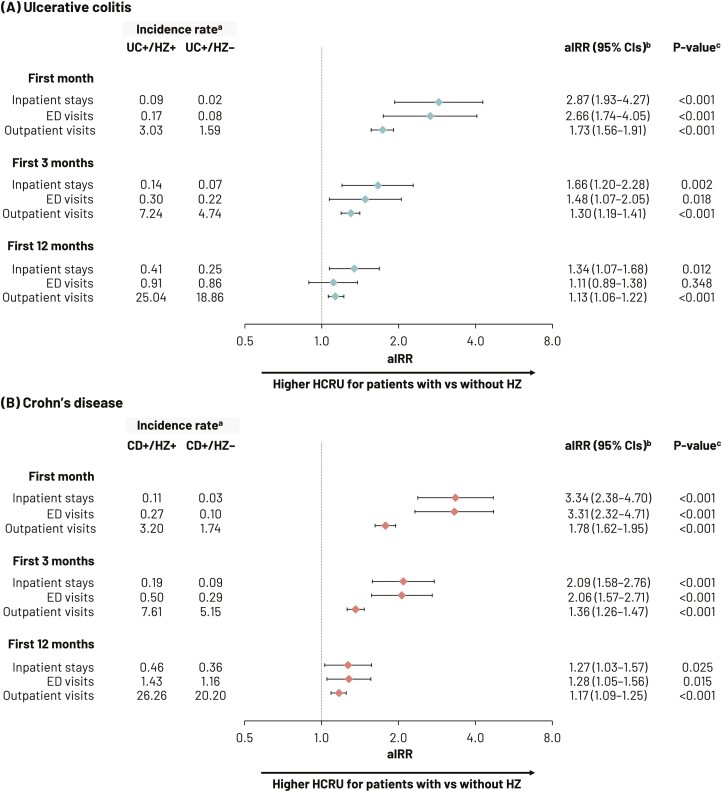
Results: In total, 20 948 patients were included: UC+/HZ+ (n = 431), UC+/HZ- (n = 10 285), CD+/HZ+ (n = 435), and CD+/HZ- (n = 9797). Patients with HZ had higher all-cause HCRU rates and all-cause total healthcare costs relative to those without HZ. In the first month, adjusted incidence rate ratios (aIRRs) for hospitalizations and ED visits for patients with UC and HZ compared with UC alone were 2.87 (95% confidence interval [CI], 1.93-4.27) and 2.66 (95% CI,1.74-4.05), respectively; for those with CD and HZ, aIRRs were 3.34 (95% CI, 2.38-4.70) and 3.31 (95% CI, 2.32-4.71), respectively, compared with CD alone (all P < .001). Adjusted cost differences in UC and CD cohorts with HZ over the first month were $2189 and $3774, respectively, chiefly driven by higher inpatient costs. The incremental impact on HCRU and costs in cohorts with HZ predominantly occurred during the first quarter following diagnosis.
Conclusions: HZ is associated with increased HCRU and costs in patients with UC and CD, especially shortly after diagnosis.

 求助内容:
求助内容: 应助结果提醒方式:
应助结果提醒方式:


