Early Warning Scores to Support Continuous Wireless Vital Sign Monitoring for Complication Prediction in Patients on Surgical Wards: Retrospective Observational Study.
Mathilde C van Rossum, Robin E M Bekhuis, Ying Wang, Johannes H Hegeman, Ellis C Folbert, Miriam M R Vollenbroek-Hutten, Cornelis J Kalkman, Ewout A Kouwenhoven, Hermie J Hermens
{"title":"Early Warning Scores to Support Continuous Wireless Vital Sign Monitoring for Complication Prediction in Patients on Surgical Wards: Retrospective Observational Study.","authors":"Mathilde C van Rossum, Robin E M Bekhuis, Ying Wang, Johannes H Hegeman, Ellis C Folbert, Miriam M R Vollenbroek-Hutten, Cornelis J Kalkman, Ewout A Kouwenhoven, Hermie J Hermens","doi":"10.2196/44483","DOIUrl":null,"url":null,"abstract":"<p><strong>Background: </strong>Wireless vital sign sensors are increasingly being used to monitor patients on surgical wards. Although early warning scores (EWSs) are the current standard for the identification of patient deterioration in a ward setting, their usefulness for continuous monitoring is unknown.</p><p><strong>Objective: </strong>This study aimed to explore the usability and predictive value of high-rate EWSs obtained from continuous vital sign recordings for early identification of postoperative complications and compares the performance of a sensor-based EWS alarm system with manual intermittent EWS measurements and threshold alarms applied to individual vital sign recordings (single-parameter alarms).</p><p><strong>Methods: </strong>Continuous vital sign measurements (heart rate, respiratory rate, blood oxygen saturation, and axillary temperature) collected with wireless sensors in patients on surgical wards were used for retrospective simulation of EWSs (sensor EWSs) for different time windows (1-240 min), adopting criteria similar to EWSs based on manual vital signs measurements (nurse EWSs). Hourly sensor EWS measurements were compared between patients with (event group: 14/46, 30%) and without (control group: 32/46, 70%) postoperative complications. In addition, alarms were simulated for the sensor EWSs using a range of alarm thresholds (1-9) and compared with alarms based on nurse EWSs and single-parameter alarms. Alarm performance was evaluated using the sensitivity to predict complications within 24 hours, daily alarm rate, and false discovery rate (FDR).</p><p><strong>Results: </strong>The hourly sensor EWSs of the event group (median 3.4, IQR 3.1-4.1) was significantly higher (P<.004) compared with the control group (median 2.8, IQR 2.4-3.2). The alarm sensitivity of the hourly sensor EWSs was the highest (80%-67%) for thresholds of 3 to 5, which was associated with alarm rates of 2 (FDR=85%) to 1.2 (FDR=83%) alarms per patient per day respectively. The sensitivity of sensor EWS-based alarms was higher than that of nurse EWS-based alarms (maximum=40%) but lower than that of single-parameter alarms (87%) for all thresholds. In contrast, the (false) alarm rates of sensor EWS-based alarms were higher than that of nurse EWS-based alarms (maximum=0.6 alarm/patient/d; FDR=80%) but lower than that of single-parameter alarms (2 alarms/patient/d; FDR=84%) for most thresholds. Alarm rates for sensor EWSs increased for shorter time windows, reaching 70 alarms per patient per day when calculated every minute.</p><p><strong>Conclusions: </strong>EWSs obtained using wireless vital sign sensors may contribute to the early recognition of postoperative complications in a ward setting, with higher alarm sensitivity compared with manual EWS measurements. Although hourly sensor EWSs provide fewer alarms compared with single-parameter alarms, high false alarm rates can be expected when calculated over shorter time spans. Further studies are recommended to optimize care escalation criteria for continuous monitoring of vital signs in a ward setting and to evaluate the effects on patient outcomes.</p>","PeriodicalId":73557,"journal":{"name":"JMIR perioperative medicine","volume":"6 ","pages":"e44483"},"PeriodicalIF":0.0000,"publicationDate":"2023-08-30","publicationTypes":"Journal Article","fieldsOfStudy":null,"isOpenAccess":false,"openAccessPdf":"https://www.ncbi.nlm.nih.gov/pmc/articles/PMC10500362/pdf/","citationCount":"0","resultStr":null,"platform":"Semanticscholar","paperid":null,"PeriodicalName":"JMIR perioperative medicine","FirstCategoryId":"1085","ListUrlMain":"https://doi.org/10.2196/44483","RegionNum":0,"RegionCategory":null,"ArticlePicture":[],"TitleCN":null,"AbstractTextCN":null,"PMCID":null,"EPubDate":"","PubModel":"","JCR":"","JCRName":"","Score":null,"Total":0}
引用次数: 0
Abstract
Background: Wireless vital sign sensors are increasingly being used to monitor patients on surgical wards. Although early warning scores (EWSs) are the current standard for the identification of patient deterioration in a ward setting, their usefulness for continuous monitoring is unknown.
Objective: This study aimed to explore the usability and predictive value of high-rate EWSs obtained from continuous vital sign recordings for early identification of postoperative complications and compares the performance of a sensor-based EWS alarm system with manual intermittent EWS measurements and threshold alarms applied to individual vital sign recordings (single-parameter alarms).
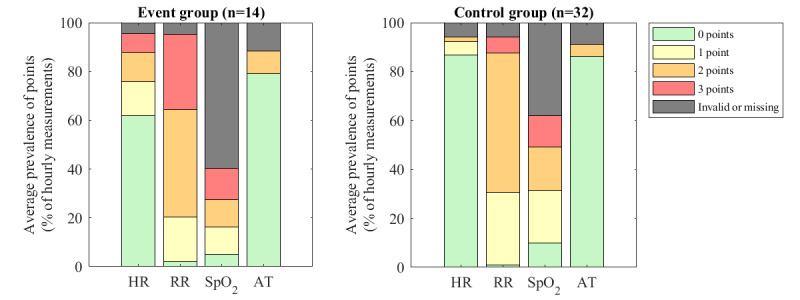
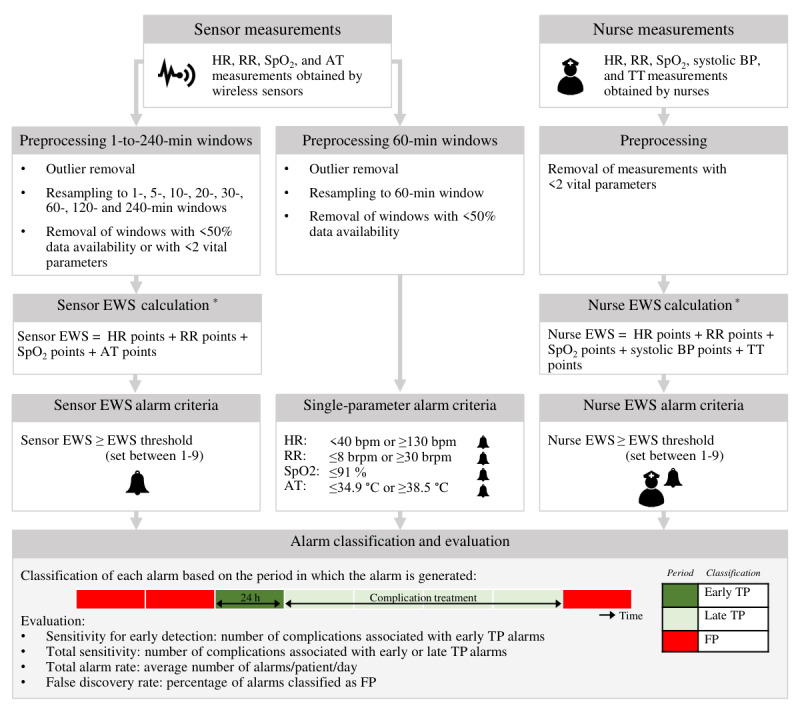
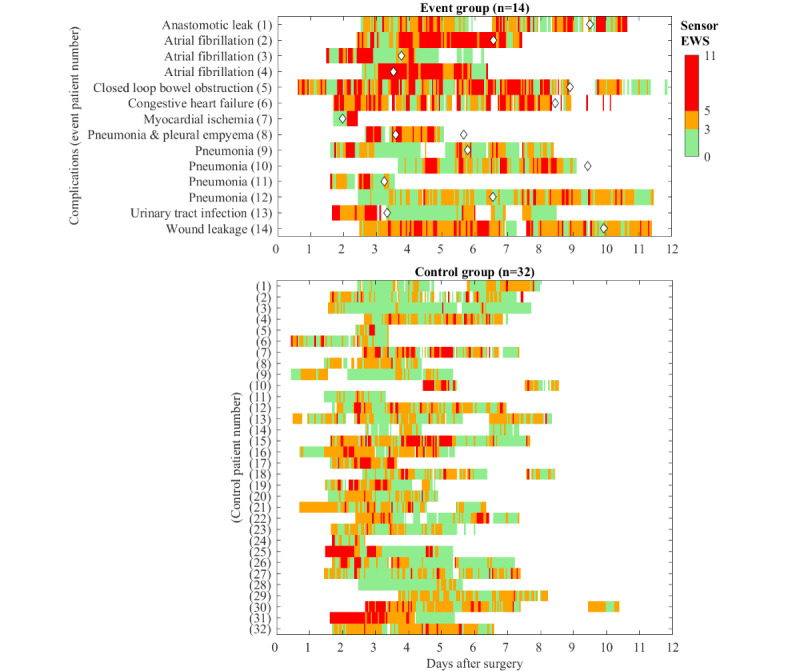
Methods: Continuous vital sign measurements (heart rate, respiratory rate, blood oxygen saturation, and axillary temperature) collected with wireless sensors in patients on surgical wards were used for retrospective simulation of EWSs (sensor EWSs) for different time windows (1-240 min), adopting criteria similar to EWSs based on manual vital signs measurements (nurse EWSs). Hourly sensor EWS measurements were compared between patients with (event group: 14/46, 30%) and without (control group: 32/46, 70%) postoperative complications. In addition, alarms were simulated for the sensor EWSs using a range of alarm thresholds (1-9) and compared with alarms based on nurse EWSs and single-parameter alarms. Alarm performance was evaluated using the sensitivity to predict complications within 24 hours, daily alarm rate, and false discovery rate (FDR).
Results: The hourly sensor EWSs of the event group (median 3.4, IQR 3.1-4.1) was significantly higher (P<.004) compared with the control group (median 2.8, IQR 2.4-3.2). The alarm sensitivity of the hourly sensor EWSs was the highest (80%-67%) for thresholds of 3 to 5, which was associated with alarm rates of 2 (FDR=85%) to 1.2 (FDR=83%) alarms per patient per day respectively. The sensitivity of sensor EWS-based alarms was higher than that of nurse EWS-based alarms (maximum=40%) but lower than that of single-parameter alarms (87%) for all thresholds. In contrast, the (false) alarm rates of sensor EWS-based alarms were higher than that of nurse EWS-based alarms (maximum=0.6 alarm/patient/d; FDR=80%) but lower than that of single-parameter alarms (2 alarms/patient/d; FDR=84%) for most thresholds. Alarm rates for sensor EWSs increased for shorter time windows, reaching 70 alarms per patient per day when calculated every minute.
Conclusions: EWSs obtained using wireless vital sign sensors may contribute to the early recognition of postoperative complications in a ward setting, with higher alarm sensitivity compared with manual EWS measurements. Although hourly sensor EWSs provide fewer alarms compared with single-parameter alarms, high false alarm rates can be expected when calculated over shorter time spans. Further studies are recommended to optimize care escalation criteria for continuous monitoring of vital signs in a ward setting and to evaluate the effects on patient outcomes.

 求助内容:
求助内容: 应助结果提醒方式:
应助结果提醒方式:


