Matthew Studham, Cristina Vazquez-Mateo, Eileen Samy, Philipp Haselmayer, Aida Aydemir, P Alexander Rolfe, Joan T Merrill, Eric F Morand, Julie DeMartino, Amy Kao, Robert Townsend
{"title":"Identifying lupus Patient Subsets Through Immune Cell Deconvolution of Gene Expression Data in Two Atacicept Phase II Studies.","authors":"Matthew Studham, Cristina Vazquez-Mateo, Eileen Samy, Philipp Haselmayer, Aida Aydemir, P Alexander Rolfe, Joan T Merrill, Eric F Morand, Julie DeMartino, Amy Kao, Robert Townsend","doi":"10.1002/acr2.11594","DOIUrl":null,"url":null,"abstract":"<p><strong>Objective: </strong>To use cell-based gene signatures to identify patients with systemic lupus erythematous (SLE) in the phase II/III APRIL-SLE and phase IIb ADDRESS II trials most likely to respond to atacicept.</p><p><strong>Methods: </strong>A published immune cell deconvolution algorithm based on Affymetrix gene array data was applied to whole blood gene expression from patients entering APRIL-SLE. Five distinct patient clusters were identified. Patient characteristics, biomarkers, and clinical response to atacicept were assessed per cluster. A modified immune cell deconvolution algorithm was developed based on RNA sequencing data and applied to ADDRESS II data to identify similar patient clusters and their responses.</p><p><strong>Results: </strong>Patients in APRIL-SLE (N = 105) were segregated into the following five clusters (P1-5) characterized by dominant cell subset signatures: high neutrophils, T helper cells and natural killer (NK) cells (P1), high plasma cells and activated NK cells (P2), high B cells and neutrophils (P3), high B cells and low neutrophils (P4), or high activated dendritic cells, activated NK cells, and neutrophils (P5). Placebo- and atacicept-treated patients in clusters P2,4,5 had markedly higher British Isles Lupus Assessment Group (BILAG) A/B flare rates than those in clusters P1,3, with a greater treatment effect of atacicept on lowering flares in clusters P2,4,5. In ADDRESS II, placebo-treated patients from P2,4,5 were less likely to be SLE Responder Index (SRI)-4, SRI-6, and BILAG-Based Combined Lupus Assessment responders than those in P1,3; the response proportions again suggested lower placebo effect and a greater treatment differential for atacicept in P2,4,5.</p><p><strong>Conclusion: </strong>This exploratory analysis indicates larger differences between placebo- and atacicept-treated patients with SLE in a molecularly defined patient subset.</p>","PeriodicalId":7084,"journal":{"name":"ACR Open Rheumatology","volume":" ","pages":"536-546"},"PeriodicalIF":0.0000,"publicationDate":"2023-10-01","publicationTypes":"Journal Article","fieldsOfStudy":null,"isOpenAccess":false,"openAccessPdf":"https://ftp.ncbi.nlm.nih.gov/pub/pmc/oa_pdf/0d/6e/ACR2-5-536.PMC10570667.pdf","citationCount":"0","resultStr":null,"platform":"Semanticscholar","paperid":null,"PeriodicalName":"ACR Open Rheumatology","FirstCategoryId":"1085","ListUrlMain":"https://doi.org/10.1002/acr2.11594","RegionNum":0,"RegionCategory":null,"ArticlePicture":[],"TitleCN":null,"AbstractTextCN":null,"PMCID":null,"EPubDate":"2023/9/14 0:00:00","PubModel":"Epub","JCR":"","JCRName":"","Score":null,"Total":0}
引用次数: 0
Abstract
Objective: To use cell-based gene signatures to identify patients with systemic lupus erythematous (SLE) in the phase II/III APRIL-SLE and phase IIb ADDRESS II trials most likely to respond to atacicept.
Methods: A published immune cell deconvolution algorithm based on Affymetrix gene array data was applied to whole blood gene expression from patients entering APRIL-SLE. Five distinct patient clusters were identified. Patient characteristics, biomarkers, and clinical response to atacicept were assessed per cluster. A modified immune cell deconvolution algorithm was developed based on RNA sequencing data and applied to ADDRESS II data to identify similar patient clusters and their responses.
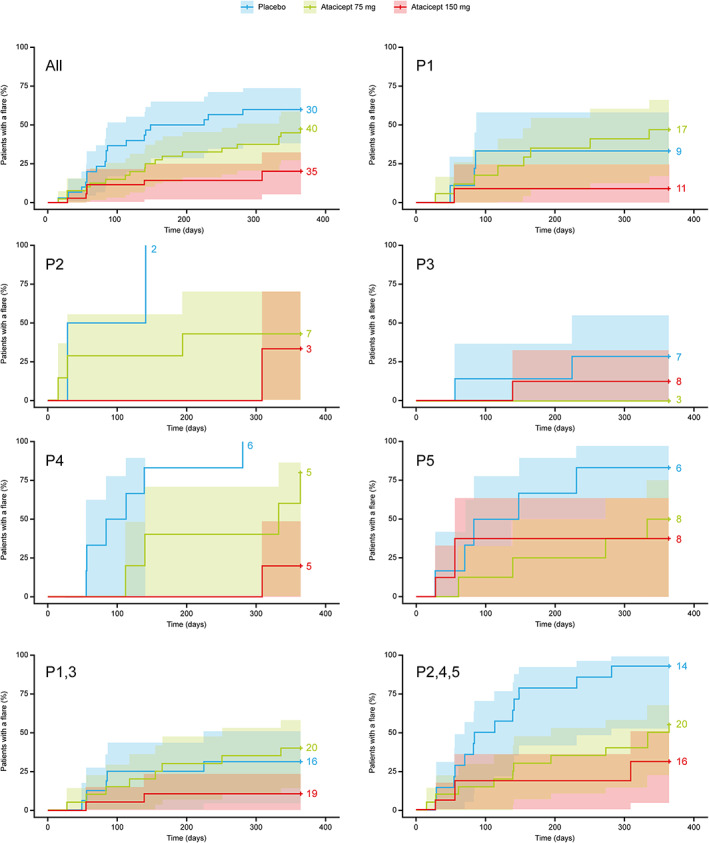
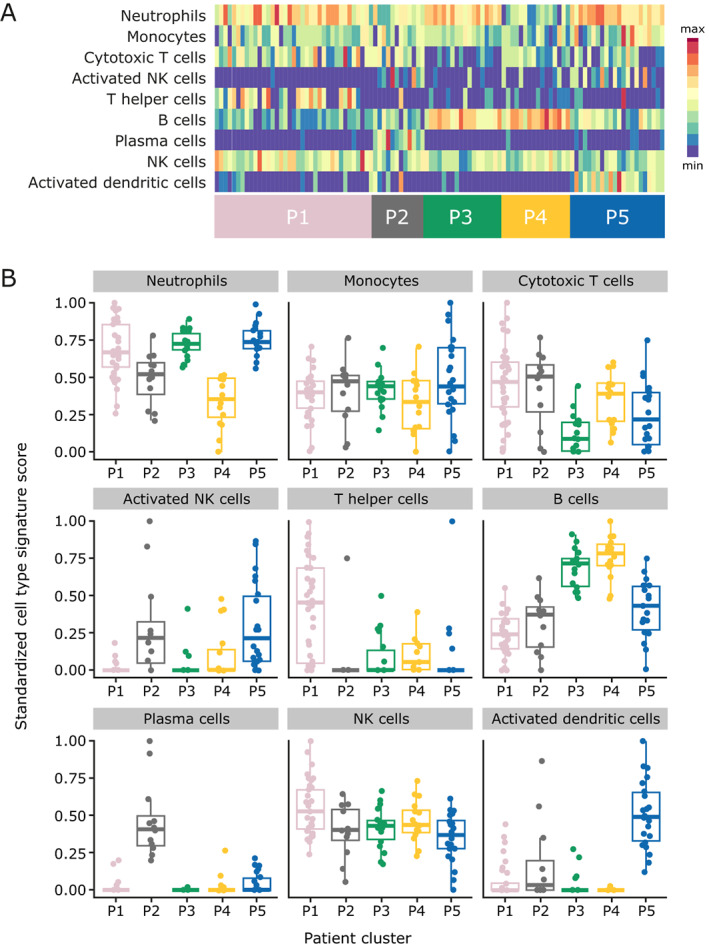
Results: Patients in APRIL-SLE (N = 105) were segregated into the following five clusters (P1-5) characterized by dominant cell subset signatures: high neutrophils, T helper cells and natural killer (NK) cells (P1), high plasma cells and activated NK cells (P2), high B cells and neutrophils (P3), high B cells and low neutrophils (P4), or high activated dendritic cells, activated NK cells, and neutrophils (P5). Placebo- and atacicept-treated patients in clusters P2,4,5 had markedly higher British Isles Lupus Assessment Group (BILAG) A/B flare rates than those in clusters P1,3, with a greater treatment effect of atacicept on lowering flares in clusters P2,4,5. In ADDRESS II, placebo-treated patients from P2,4,5 were less likely to be SLE Responder Index (SRI)-4, SRI-6, and BILAG-Based Combined Lupus Assessment responders than those in P1,3; the response proportions again suggested lower placebo effect and a greater treatment differential for atacicept in P2,4,5.
Conclusion: This exploratory analysis indicates larger differences between placebo- and atacicept-treated patients with SLE in a molecularly defined patient subset.

 求助内容:
求助内容: 应助结果提醒方式:
应助结果提醒方式:


