Association between diaphragmatic dysfunction after adult cardiovascular surgery and prognosis of mechanical ventilation: a retrospective cohort study.
{"title":"Association between diaphragmatic dysfunction after adult cardiovascular surgery and prognosis of mechanical ventilation: a retrospective cohort study.","authors":"Reimi Inoue, Yusuke Nagamine, Masahide Ohtsuka, Takahisa Goto","doi":"10.1186/s40560-023-00688-x","DOIUrl":null,"url":null,"abstract":"<p><strong>Background: </strong>Diaphragmatic dysfunction often occurs after adult cardiovascular surgery. The prognostic effect of diaphragmatic dysfunction on ventilatory management in patients after cardiovascular surgery is unknown. This study aimed to investigate the association between diaphragmatic dysfunction and prognosis of ventilatory management in adult postoperative cardiovascular surgery patients.</p><p><strong>Methods: </strong>This study was a single-center retrospective cohort study conducted at a tertiary care university hospital. This study included adult patients admitted to the intensive care unit under tracheal intubation after cardiovascular surgery. Spontaneous breathing trial was performed, and bilateral diaphragmatic motion was assessed using ultrasonography; diaphragmatic dysfunction was classified as normal, incomplete dysfunction, or complete dysfunction. The primary outcome was weaning off in mechanical ventilation. The duration of mechanical ventilation was defined as duration from the date of ICU admission to the date of weaning off in mechanical ventilation. The secondary outcomes were reintubation, death from all causes, improvement of diaphragm position assessed by chest radiographs. The subdistribution hazard ratio or hazard ratio (HR) with 95% confidence of intervals (CIs) were estimated by Fine-Gray models or Cox proportional hazard models adjusted for potential confounders.</p><p><strong>Results: </strong>Of 153 patients analyzed, 49 patients (32.0%) had diaphragmatic dysfunction. Diaphragmatic dysfunction consisted of incomplete dysfunction in 38 patients and complete dysfunction in 11 patients. Diaphragmatic dysfunction groups had longer duration of mechanical ventilation (68 h [interquartile range (IQR) 39-114] vs 23 h [15-67], adjusted subdistribution HR 0.63, 95% CIs 0.43-0.92). There was a higher rate of reintubation (12.2% vs 2.9%, univariate logistic regression analysis p = 0.034, unadjusted odds ratio = 4.70, 95% CIs 1.12-19.65), and a tendency to have higher death from all causes in the diaphragmatic dysfunction group during follow-up period (maximum 6.5 years) (18.4% vs 9.6%, adjusted HR 1.64, 95% CIs 0.59-4.53). The time to improvement of diaphragm position on chest radiograph was significantly longer in the diaphragmatic dysfunction group (14 days [IQR 6-29] vs 5 days [IQR 2-10], adjusted subdistribution HR 0.54, 95% CIs 0.38-0.77).</p><p><strong>Conclusions: </strong>Diaphragmatic dysfunction after adult cardiovascular surgery was significantly associated with longer duration of mechanical ventilation and higher reintubation.</p>","PeriodicalId":16123,"journal":{"name":"Journal of Intensive Care","volume":"11 1","pages":"39"},"PeriodicalIF":3.8000,"publicationDate":"2023-09-12","publicationTypes":"Journal Article","fieldsOfStudy":null,"isOpenAccess":false,"openAccessPdf":"https://www.ncbi.nlm.nih.gov/pmc/articles/PMC10496287/pdf/","citationCount":"0","resultStr":null,"platform":"Semanticscholar","paperid":null,"PeriodicalName":"Journal of Intensive Care","FirstCategoryId":"3","ListUrlMain":"https://doi.org/10.1186/s40560-023-00688-x","RegionNum":2,"RegionCategory":"医学","ArticlePicture":[],"TitleCN":null,"AbstractTextCN":null,"PMCID":null,"EPubDate":"","PubModel":"","JCR":"Q1","JCRName":"CRITICAL CARE MEDICINE","Score":null,"Total":0}
引用次数: 0
Abstract
Background: Diaphragmatic dysfunction often occurs after adult cardiovascular surgery. The prognostic effect of diaphragmatic dysfunction on ventilatory management in patients after cardiovascular surgery is unknown. This study aimed to investigate the association between diaphragmatic dysfunction and prognosis of ventilatory management in adult postoperative cardiovascular surgery patients.
Methods: This study was a single-center retrospective cohort study conducted at a tertiary care university hospital. This study included adult patients admitted to the intensive care unit under tracheal intubation after cardiovascular surgery. Spontaneous breathing trial was performed, and bilateral diaphragmatic motion was assessed using ultrasonography; diaphragmatic dysfunction was classified as normal, incomplete dysfunction, or complete dysfunction. The primary outcome was weaning off in mechanical ventilation. The duration of mechanical ventilation was defined as duration from the date of ICU admission to the date of weaning off in mechanical ventilation. The secondary outcomes were reintubation, death from all causes, improvement of diaphragm position assessed by chest radiographs. The subdistribution hazard ratio or hazard ratio (HR) with 95% confidence of intervals (CIs) were estimated by Fine-Gray models or Cox proportional hazard models adjusted for potential confounders.
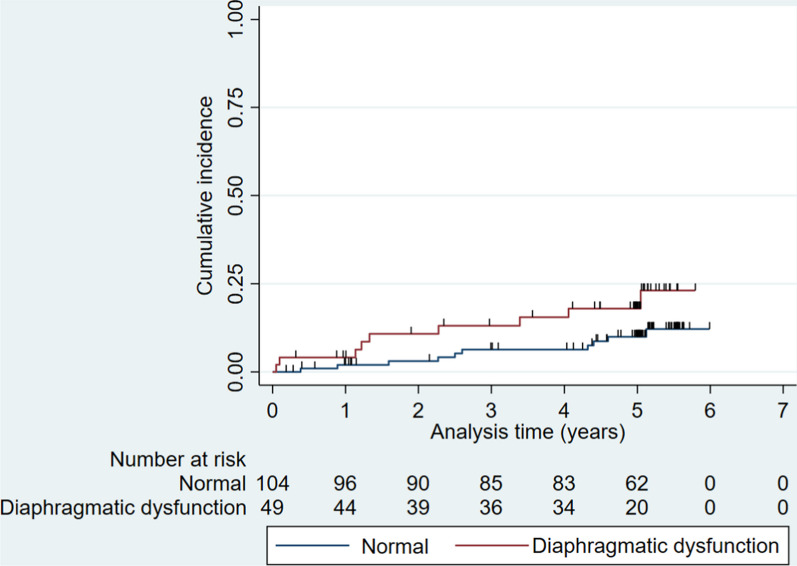
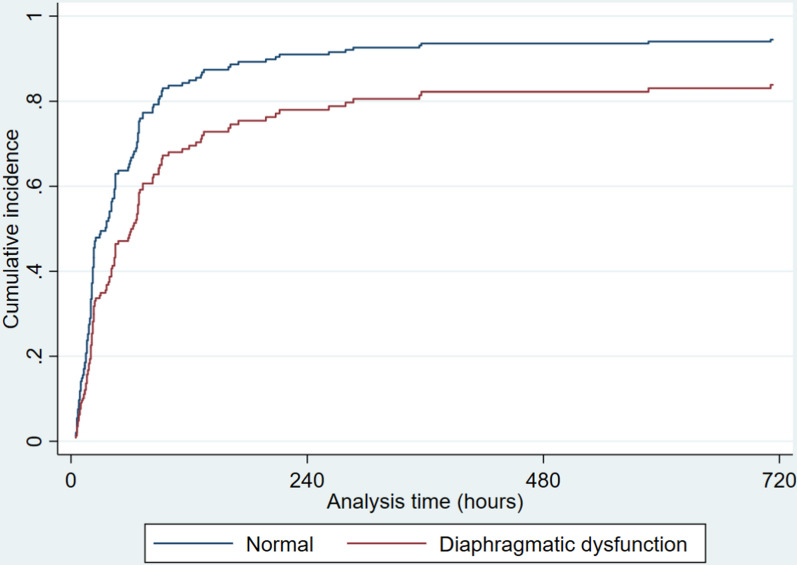
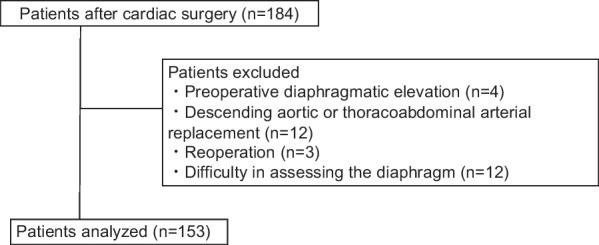
Results: Of 153 patients analyzed, 49 patients (32.0%) had diaphragmatic dysfunction. Diaphragmatic dysfunction consisted of incomplete dysfunction in 38 patients and complete dysfunction in 11 patients. Diaphragmatic dysfunction groups had longer duration of mechanical ventilation (68 h [interquartile range (IQR) 39-114] vs 23 h [15-67], adjusted subdistribution HR 0.63, 95% CIs 0.43-0.92). There was a higher rate of reintubation (12.2% vs 2.9%, univariate logistic regression analysis p = 0.034, unadjusted odds ratio = 4.70, 95% CIs 1.12-19.65), and a tendency to have higher death from all causes in the diaphragmatic dysfunction group during follow-up period (maximum 6.5 years) (18.4% vs 9.6%, adjusted HR 1.64, 95% CIs 0.59-4.53). The time to improvement of diaphragm position on chest radiograph was significantly longer in the diaphragmatic dysfunction group (14 days [IQR 6-29] vs 5 days [IQR 2-10], adjusted subdistribution HR 0.54, 95% CIs 0.38-0.77).
Conclusions: Diaphragmatic dysfunction after adult cardiovascular surgery was significantly associated with longer duration of mechanical ventilation and higher reintubation.
背景:成人心血管手术后常发生膈肌功能障碍。心血管手术后膈功能障碍对患者通气管理的预后影响尚不清楚。本研究旨在探讨成人心血管术后患者膈功能障碍与通气管理预后的关系。方法:本研究是一项在大学三级医院进行的单中心回顾性队列研究。本研究包括心血管手术后气管插管入住重症监护病房的成年患者。进行自主呼吸试验,超声检查双侧膈肌运动;膈功能障碍分为正常、不完全功能障碍和完全功能障碍。主要结果是机械通气脱机。机械通气持续时间定义为从患者入ICU至机械通气停机的持续时间。次要结果为重新插管、各种原因死亡、胸片评估膈肌位置的改善。95%置信区间(ci)的亚分布风险比或风险比(HR)通过Fine-Gray模型或Cox比例风险模型对潜在混杂因素进行校正。结果:153例患者中,49例(32.0%)存在膈功能障碍。膈功能障碍包括38例不完全功能障碍和11例完全功能障碍。膈功能障碍组机械通气持续时间较长(68 h[四分位间距(IQR) 39-114] vs 23 h[15-67],调整后亚分布HR 0.63, 95% ci 0.43-0.92)。在随访期间(最长6.5年),膈功能障碍组的再插管率较高(12.2% vs 2.9%,单因素logistic回归分析p = 0.034,未经校正的优势比= 4.70,95% ci 1.12-19.65),且各种原因导致的死亡率有较高的趋势(18.4% vs 9.6%,校正HR 1.64, 95% ci 0.59-4.53)。膈功能障碍组胸片膈位置改善所需时间明显更长(14天[IQR 6-29] vs 5天[IQR 2-10],调整后亚分布HR 0.54, 95% ci 0.38-0.77)。结论:成人心血管手术后膈肌功能障碍与较长的机械通气时间和较高的再插管次数显著相关。
期刊介绍:
"Journal of Intensive Care" is an open access journal dedicated to the comprehensive coverage of intensive care medicine, providing a platform for the latest research and clinical insights in this critical field. The journal covers a wide range of topics, including intensive and critical care, trauma and surgical intensive care, pediatric intensive care, acute and emergency medicine, perioperative medicine, resuscitation, infection control, and organ dysfunction.
Recognizing the importance of cultural diversity in healthcare practices, "Journal of Intensive Care" also encourages submissions that explore and discuss the cultural aspects of intensive care, aiming to promote a more inclusive and culturally sensitive approach to patient care. By fostering a global exchange of knowledge and expertise, the journal contributes to the continuous improvement of intensive care practices worldwide.

 求助内容:
求助内容: 应助结果提醒方式:
应助结果提醒方式:


