{"title":"Beta-blocker therapy in patients with acute myocardial infarction: not all patients need it.","authors":"Seung-Jae Joo","doi":"10.4266/acc.2023.00955","DOIUrl":null,"url":null,"abstract":"<p><p>Most of the evidences for beneficial effects of beta-blockers in patients with acute myocardial infarction (AMI) were from the clinical studies published in the pre-reperfusion era when anti-platelet drugs, statins or inhibitors of renin-angiotensin-aldosterone system which are known to reduce cardiovascular mortality of patients with AMI were not introduced. In the reperfusion era, beta-blockers' benefit has not been clearly shown except in patients with reduced ejection fraction (EF; ≤40%). In the era of the early reperfusion therapy for AMI, a number of patients with mildly reduced EF (>40%, <50%) or preserved EF (≥50%) become increasing. However, because no randomized clinical trials are available until now, the benefit and the optimal duration of oral treatment with beta-blockers in patients with mildly reduced or preserved EF are questionable. Registry data have not showed the association of oral beta-blocker therapy with decreased mortality in survivors without heart failure or left ventricular systolic dysfunction after AMI. In the Korea Acute Myocardial Infarction Registry-National Institute of Health of in-hospital survivors after AMI, the benefit of beta-blocker therapy at discharge was shown in patients with reduced or mildly reduced EF, but not in those with preserved EF, which provides new information about beta-blocker therapy in patients without reduced EF. However, clinical practice can be changed when the results of appropriate randomized clinical trials are available. Ongoing clinical trials may help to answer the unresolved issues of beta-blocker therapy in patients with AMI.</p>","PeriodicalId":44118,"journal":{"name":"Acute and Critical Care","volume":"38 3","pages":"251-260"},"PeriodicalIF":1.7000,"publicationDate":"2023-08-01","publicationTypes":"Journal Article","fieldsOfStudy":null,"isOpenAccess":false,"openAccessPdf":"https://ftp.ncbi.nlm.nih.gov/pub/pmc/oa_pdf/54/5a/acc-2023-00955.PMC10497890.pdf","citationCount":"0","resultStr":null,"platform":"Semanticscholar","paperid":null,"PeriodicalName":"Acute and Critical Care","FirstCategoryId":"1085","ListUrlMain":"https://doi.org/10.4266/acc.2023.00955","RegionNum":0,"RegionCategory":null,"ArticlePicture":[],"TitleCN":null,"AbstractTextCN":null,"PMCID":null,"EPubDate":"2023/8/31 0:00:00","PubModel":"Epub","JCR":"Q3","JCRName":"CRITICAL CARE MEDICINE","Score":null,"Total":0}
引用次数: 0
Abstract
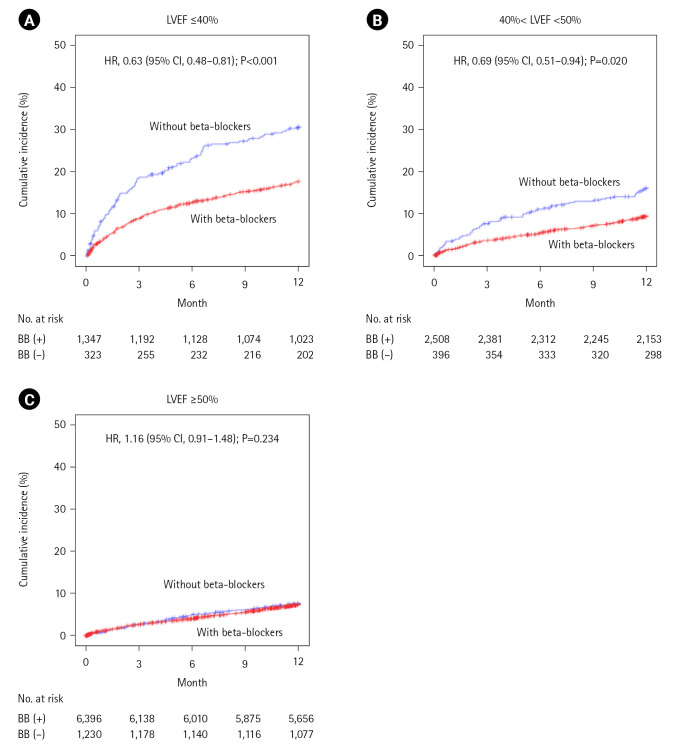
Most of the evidences for beneficial effects of beta-blockers in patients with acute myocardial infarction (AMI) were from the clinical studies published in the pre-reperfusion era when anti-platelet drugs, statins or inhibitors of renin-angiotensin-aldosterone system which are known to reduce cardiovascular mortality of patients with AMI were not introduced. In the reperfusion era, beta-blockers' benefit has not been clearly shown except in patients with reduced ejection fraction (EF; ≤40%). In the era of the early reperfusion therapy for AMI, a number of patients with mildly reduced EF (>40%, <50%) or preserved EF (≥50%) become increasing. However, because no randomized clinical trials are available until now, the benefit and the optimal duration of oral treatment with beta-blockers in patients with mildly reduced or preserved EF are questionable. Registry data have not showed the association of oral beta-blocker therapy with decreased mortality in survivors without heart failure or left ventricular systolic dysfunction after AMI. In the Korea Acute Myocardial Infarction Registry-National Institute of Health of in-hospital survivors after AMI, the benefit of beta-blocker therapy at discharge was shown in patients with reduced or mildly reduced EF, but not in those with preserved EF, which provides new information about beta-blocker therapy in patients without reduced EF. However, clinical practice can be changed when the results of appropriate randomized clinical trials are available. Ongoing clinical trials may help to answer the unresolved issues of beta-blocker therapy in patients with AMI.

 求助内容:
求助内容: 应助结果提醒方式:
应助结果提醒方式:


