Khaoula Ben Ismail, Fatma Essafi, Imen Talik, Najla Ben Slimene, Ines Sdiri, Boudour Ben Dhia, Takoua Merhbene
{"title":"Awake prone positioning for COVID-19 acute hypoxemic respiratory failure in Tunisia.","authors":"Khaoula Ben Ismail, Fatma Essafi, Imen Talik, Najla Ben Slimene, Ines Sdiri, Boudour Ben Dhia, Takoua Merhbene","doi":"10.4266/acc.2023.00591","DOIUrl":null,"url":null,"abstract":"<p><strong>Background: </strong>In this study, we explored whether awake prone position (PP) can impact prognosis of severe hypoxemia coronavirus disease 2019 (COVID-19) patients.</p><p><strong>Methods: </strong>This was a prospective observational study of severe, critically ill adult COVID-19 patients admitted to the intensive care unit. Patients were divided into two groups: group G1, patients who benefited from a vigilant and effective PP (>4 hours minimum/24) and group G2, control group. We compared demographic, clinical, paraclinical and evolutionary data.</p><p><strong>Results: </strong>Three hundred forty-nine patients were hospitalized during the study period, 273 met the inclusion criteria. PP was performed in 192 patients (70.3%). The two groups were comparable in terms of demographic characteristics, clinical severity and modalities of oxygenation at intensive care unit (ICU) admission. The mean PaO2/ FIO2 ratios were 141 and 128 mm Hg, respectively (P=0.07). The computed tomography scan was comparable with a critical >75% in 48.5% (G1) versus 54.2% (G2). The median duration of the daily PP session was 13±7 hours per day. The average duration of spontaneous PP days was 7 days (4-19). Use of invasive ventilation was lower in the G1 group (27% vs. 56%, P=0.002). Healthcare-associated infections were significantly lower in G1 (42.1% vs. 82%, P=0.01). Duration of total mechanical ventilation and length of ICU stay were comparable between the two groups. Mortality was significantly higher in G2 (64% vs. 28%, P=0.02).</p><p><strong>Conclusions: </strong>Our study confirmed that awake PP can improve prognosis in COVID-19 patients. Randomized controlled trials are needed to confirm this result.</p>","PeriodicalId":44118,"journal":{"name":"Acute and Critical Care","volume":null,"pages":null},"PeriodicalIF":1.7000,"publicationDate":"2023-08-01","publicationTypes":"Journal Article","fieldsOfStudy":null,"isOpenAccess":false,"openAccessPdf":"https://ftp.ncbi.nlm.nih.gov/pub/pmc/oa_pdf/b1/97/acc-2023-00591.PMC10497894.pdf","citationCount":"0","resultStr":null,"platform":"Semanticscholar","paperid":null,"PeriodicalName":"Acute and Critical Care","FirstCategoryId":"1085","ListUrlMain":"https://doi.org/10.4266/acc.2023.00591","RegionNum":0,"RegionCategory":null,"ArticlePicture":[],"TitleCN":null,"AbstractTextCN":null,"PMCID":null,"EPubDate":"","PubModel":"","JCR":"Q3","JCRName":"CRITICAL CARE MEDICINE","Score":null,"Total":0}
引用次数: 0
Abstract
Background: In this study, we explored whether awake prone position (PP) can impact prognosis of severe hypoxemia coronavirus disease 2019 (COVID-19) patients.
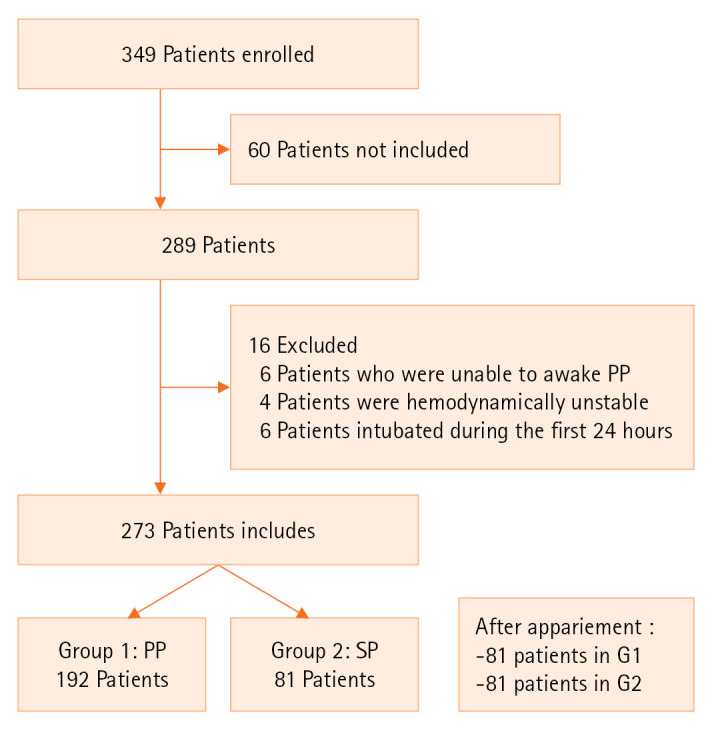
Methods: This was a prospective observational study of severe, critically ill adult COVID-19 patients admitted to the intensive care unit. Patients were divided into two groups: group G1, patients who benefited from a vigilant and effective PP (>4 hours minimum/24) and group G2, control group. We compared demographic, clinical, paraclinical and evolutionary data.
Results: Three hundred forty-nine patients were hospitalized during the study period, 273 met the inclusion criteria. PP was performed in 192 patients (70.3%). The two groups were comparable in terms of demographic characteristics, clinical severity and modalities of oxygenation at intensive care unit (ICU) admission. The mean PaO2/ FIO2 ratios were 141 and 128 mm Hg, respectively (P=0.07). The computed tomography scan was comparable with a critical >75% in 48.5% (G1) versus 54.2% (G2). The median duration of the daily PP session was 13±7 hours per day. The average duration of spontaneous PP days was 7 days (4-19). Use of invasive ventilation was lower in the G1 group (27% vs. 56%, P=0.002). Healthcare-associated infections were significantly lower in G1 (42.1% vs. 82%, P=0.01). Duration of total mechanical ventilation and length of ICU stay were comparable between the two groups. Mortality was significantly higher in G2 (64% vs. 28%, P=0.02).
Conclusions: Our study confirmed that awake PP can improve prognosis in COVID-19 patients. Randomized controlled trials are needed to confirm this result.

 求助内容:
求助内容: 应助结果提醒方式:
应助结果提醒方式:


