Shelly L Gray, Subashan Perera, Tim Soverns, Joseph T Hanlon
{"title":"Systematic Review and Meta-analysis of Interventions to Reduce Adverse Drug Reactions in Older Adults: An Update.","authors":"Shelly L Gray, Subashan Perera, Tim Soverns, Joseph T Hanlon","doi":"10.1007/s40266-023-01064-y","DOIUrl":null,"url":null,"abstract":"<p><strong>Background: </strong>We previously reported that interventions to optimize medication use reduced adverse drug reactions (ADRs) by 21% and serious ADRs by 36% in older adults. With new evidence, we sought to update the systematic review and meta-analysis.</p><p><strong>Method: </strong>We searched OVID, Cochrane Library, ClinicalTrials.gov and Google Scholar from 30 April 2017-30 April 2023. Included studies had to be randomized controlled trials of older adults (mean age ≥65 years) taking medications that examined the outcome of ADRs. Two authors independently reviewed all citations, extracted relevant data, and assessed studies for potential bias. The outcomes were any and serious ADRs. We performed subgroup analyses by intervention type and setting. Random-effects models were used to combine the results from multiple studies and create summary estimates.</p><p><strong>Results: </strong>Six studies are new to the update, resulting in 19 total studies (15,675 participants). Interventions were pharmacist-led (10 studies), other healthcare professional-led (5 studies), technology based (3 studies), and educational (1 study). The interventions were implemented in various clinical settings, including hospitals, outpatient clinics, long-term care facilities/rehabilitation wards, and community pharmacies. In the pooled analysis, the intervention group participants were 19% less likely to experience an ADR (odds ratio [OR] 0.81, 95% confidence interval [CI] 0.68-0.96) and 32% less likely to experience a serious ADR (OR 0.68, 95% CI 0.48-0.96). We also found that pharmacist-led interventions reduced the risk of any ADR by 35%, compared with 8% for other types of interventions.</p><p><strong>Conclusion: </strong>Interventions significantly and substantially reduced the risk of ADRs and serious ADRs in older adults. Future research should examine whether effectiveness of interventions vary across health care settings to identify those most likely to benefit. Implementation of successful interventions in health care systems may improve medication safety in older patients.</p>","PeriodicalId":11489,"journal":{"name":"Drugs & Aging","volume":null,"pages":null},"PeriodicalIF":3.4000,"publicationDate":"2023-11-01","publicationTypes":"Journal Article","fieldsOfStudy":null,"isOpenAccess":false,"openAccessPdf":"https://ftp.ncbi.nlm.nih.gov/pub/pmc/oa_pdf/ab/a5/40266_2023_Article_1064.PMC10600043.pdf","citationCount":"0","resultStr":null,"platform":"Semanticscholar","paperid":null,"PeriodicalName":"Drugs & Aging","FirstCategoryId":"3","ListUrlMain":"https://doi.org/10.1007/s40266-023-01064-y","RegionNum":3,"RegionCategory":"医学","ArticlePicture":[],"TitleCN":null,"AbstractTextCN":null,"PMCID":null,"EPubDate":"2023/9/13 0:00:00","PubModel":"Epub","JCR":"Q2","JCRName":"GERIATRICS & GERONTOLOGY","Score":null,"Total":0}
引用次数: 0
Abstract
Background: We previously reported that interventions to optimize medication use reduced adverse drug reactions (ADRs) by 21% and serious ADRs by 36% in older adults. With new evidence, we sought to update the systematic review and meta-analysis.
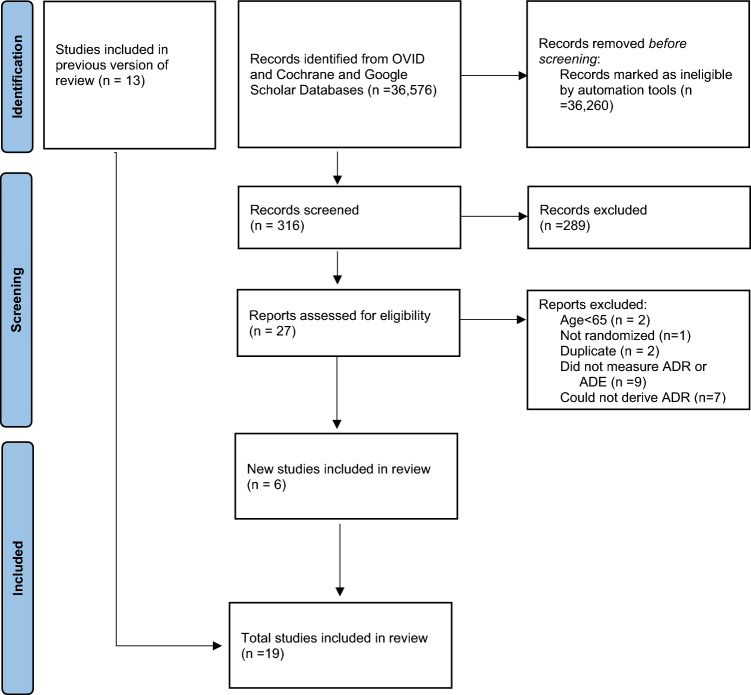
Method: We searched OVID, Cochrane Library, ClinicalTrials.gov and Google Scholar from 30 April 2017-30 April 2023. Included studies had to be randomized controlled trials of older adults (mean age ≥65 years) taking medications that examined the outcome of ADRs. Two authors independently reviewed all citations, extracted relevant data, and assessed studies for potential bias. The outcomes were any and serious ADRs. We performed subgroup analyses by intervention type and setting. Random-effects models were used to combine the results from multiple studies and create summary estimates.
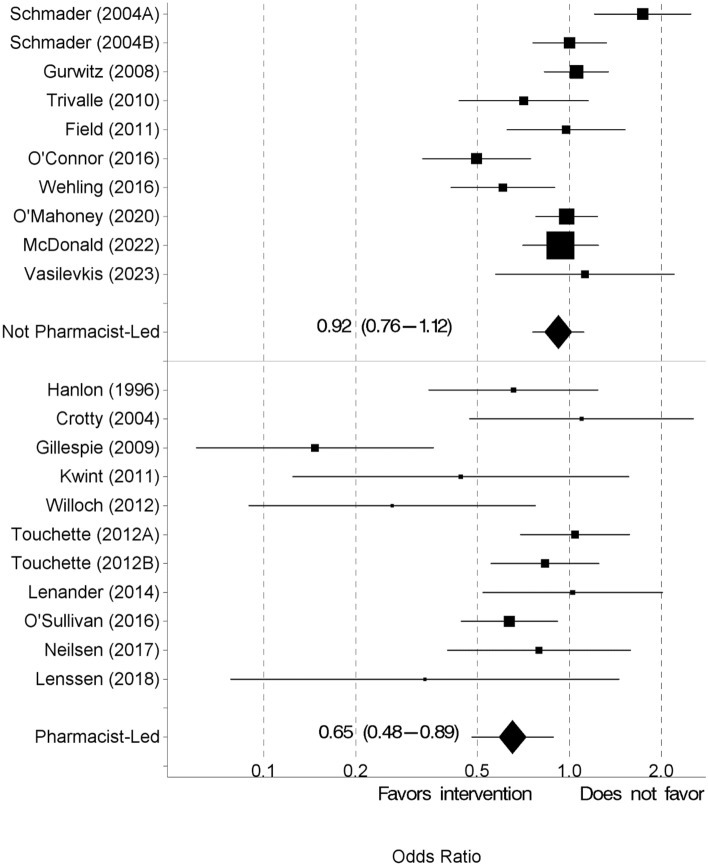
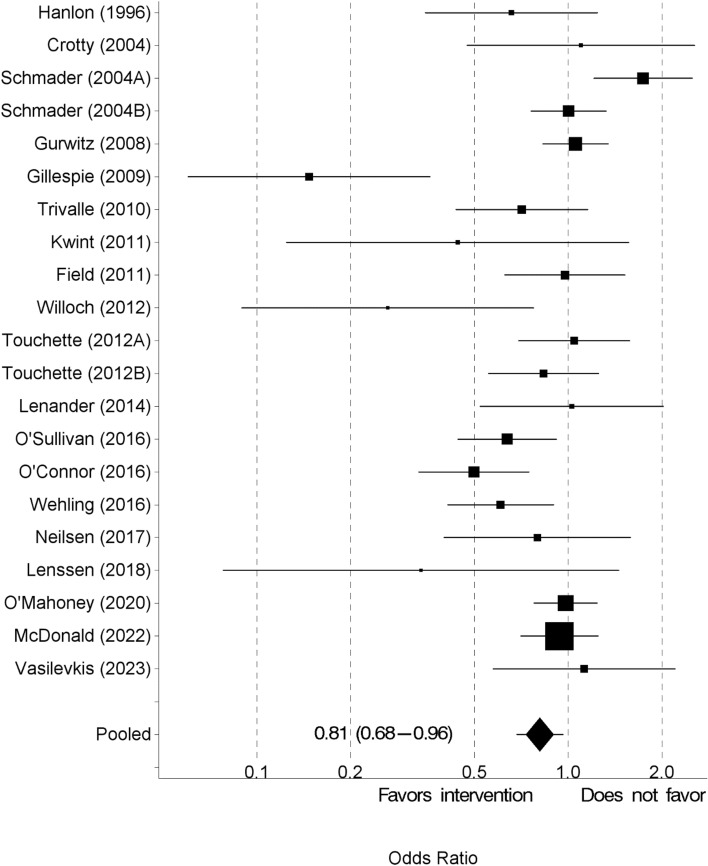
Results: Six studies are new to the update, resulting in 19 total studies (15,675 participants). Interventions were pharmacist-led (10 studies), other healthcare professional-led (5 studies), technology based (3 studies), and educational (1 study). The interventions were implemented in various clinical settings, including hospitals, outpatient clinics, long-term care facilities/rehabilitation wards, and community pharmacies. In the pooled analysis, the intervention group participants were 19% less likely to experience an ADR (odds ratio [OR] 0.81, 95% confidence interval [CI] 0.68-0.96) and 32% less likely to experience a serious ADR (OR 0.68, 95% CI 0.48-0.96). We also found that pharmacist-led interventions reduced the risk of any ADR by 35%, compared with 8% for other types of interventions.
Conclusion: Interventions significantly and substantially reduced the risk of ADRs and serious ADRs in older adults. Future research should examine whether effectiveness of interventions vary across health care settings to identify those most likely to benefit. Implementation of successful interventions in health care systems may improve medication safety in older patients.
期刊介绍:
Drugs & Aging delivers essential information on the most important aspects of drug therapy to professionals involved in the care of the elderly.
The journal addresses in a timely way the major issues relating to drug therapy in older adults including: the management of specific diseases, particularly those associated with aging, age-related physiological changes impacting drug therapy, drug utilization and prescribing in the elderly, polypharmacy and drug interactions.

 求助内容:
求助内容: 应助结果提醒方式:
应助结果提醒方式:


