{"title":"Minimal invasive extracorporeal circulation an alternative to ECMO in ventricular tachycardia ablation.","authors":"Ignazio Condello","doi":"10.1051/ject/2023031","DOIUrl":null,"url":null,"abstract":"<p><strong>Background: </strong>The advantages of mechanical assistance during ventricular tachycardia (VT) ablation have not been clinically demonstrated. We propose and discuss a technique, set up by us, that makes use of minimally invasive extra-corporeal circulation (MiECC) type III associated with a venous reservoir system, which allows complete cardiac flow support and blood oxygenation as well as hemodynamic stability during long-lasting procedures.</p><p><strong>Methods: </strong>We present a retrospective case series of ten patients with valvular heart disease and unresponsive Ventricular Tachycardia (VT) who underwent VT ablation with MiECC support. The mean age of the patients was 72 ± 8 years and the left ventricular ejection fraction was 36 ± 12%. All patients underwent a clinical evaluation to identify the cause of VT unresponsiveness (e.g., ischemic heart disease).</p><p><strong>Results: </strong>A total of 140 min, the following parameters were evaluated and recorded for 140 min. Central venous pressure (CVP) was used to evaluate excess volume. During the first 5 min, the mean was 15 mmHg, with a pump flow of 1.5 L/min and a mean systemic arterial pressure of 100 mmHg while setting up the circulation support. Following drainage in a volumetric bag of 1 L of blood, CVP was reduced to a value of 5 mmHg with a flow rate of 5 L/min and a mean systemic arterial pressure of 65 mmHg. In the case of small and low-weight patients our \"1 L protocol\" can be modified.</p><p><strong>Conclusions: </strong>In this preliminary retrospective case series, the MiECC type III system may represent the ideal support system during VT ablation, and further studies are needed to support this preliminary report.</p>","PeriodicalId":39644,"journal":{"name":"Journal of Extra-Corporeal Technology","volume":"55 3","pages":"138-143"},"PeriodicalIF":0.0000,"publicationDate":"2023-09-01","publicationTypes":"Journal Article","fieldsOfStudy":null,"isOpenAccess":false,"openAccessPdf":"https://www.ncbi.nlm.nih.gov/pmc/articles/PMC10487307/pdf/","citationCount":"0","resultStr":null,"platform":"Semanticscholar","paperid":null,"PeriodicalName":"Journal of Extra-Corporeal Technology","FirstCategoryId":"1085","ListUrlMain":"https://doi.org/10.1051/ject/2023031","RegionNum":0,"RegionCategory":null,"ArticlePicture":[],"TitleCN":null,"AbstractTextCN":null,"PMCID":null,"EPubDate":"","PubModel":"","JCR":"Q2","JCRName":"Health Professions","Score":null,"Total":0}
引用次数: 0
Abstract
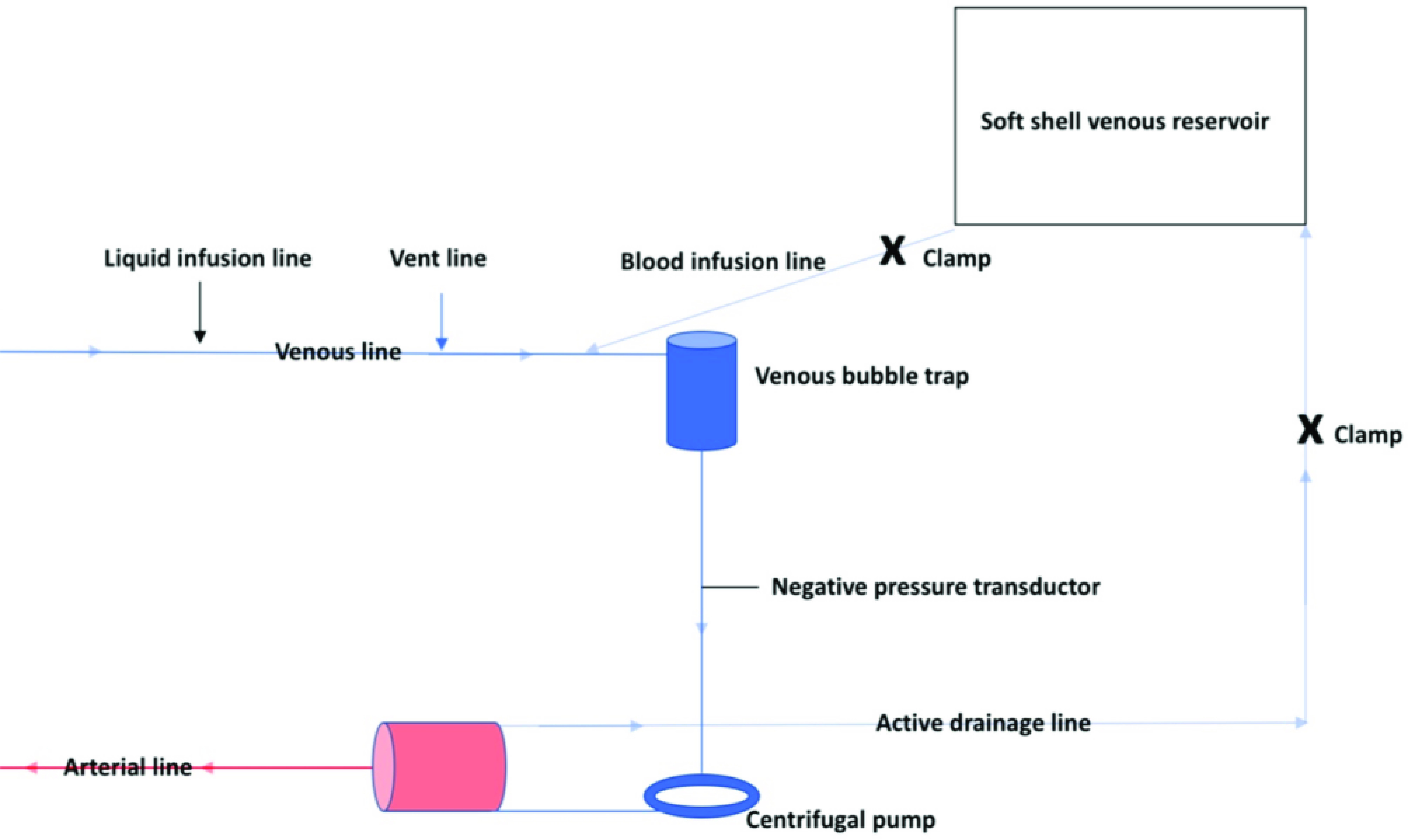
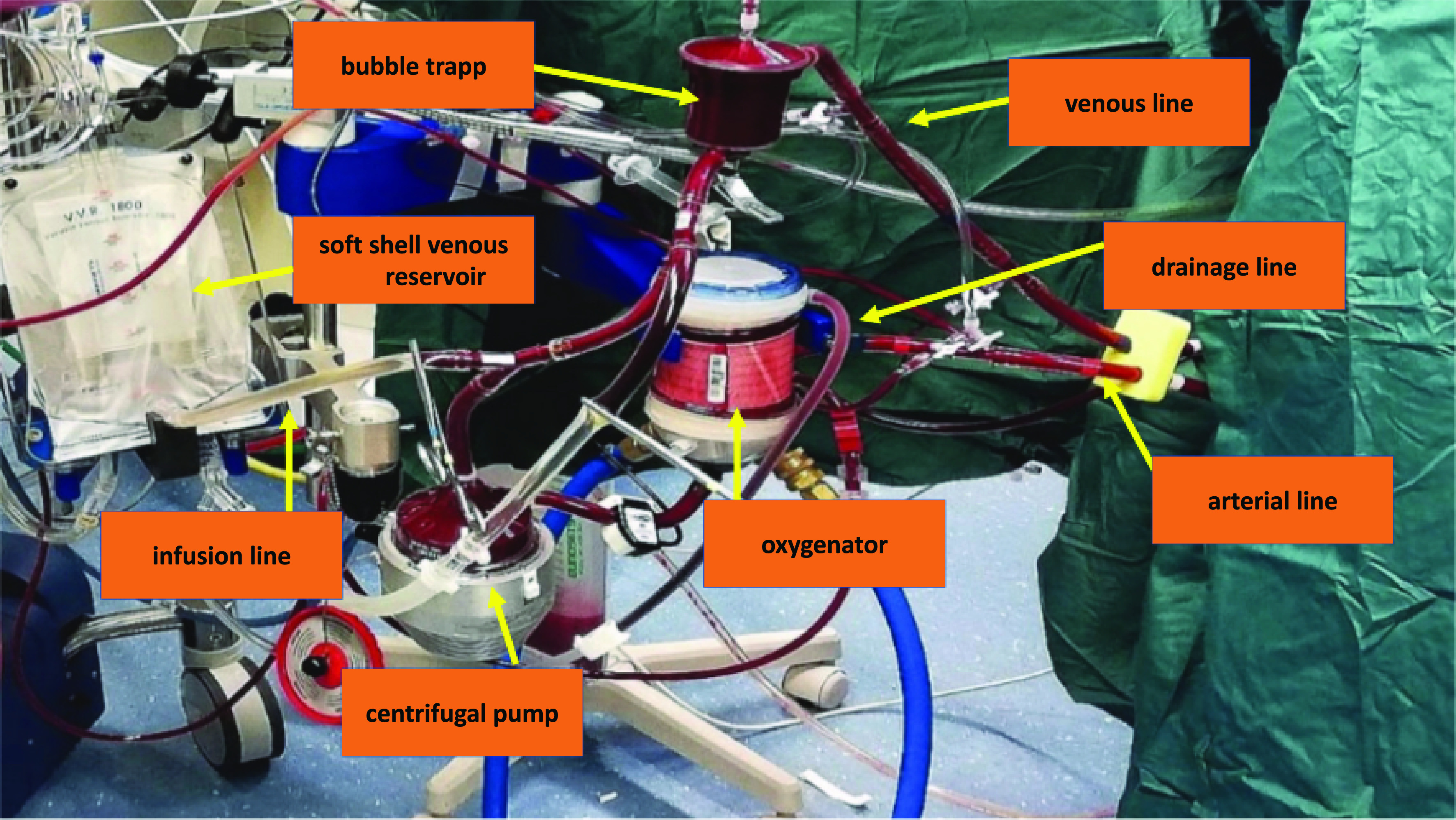
Background: The advantages of mechanical assistance during ventricular tachycardia (VT) ablation have not been clinically demonstrated. We propose and discuss a technique, set up by us, that makes use of minimally invasive extra-corporeal circulation (MiECC) type III associated with a venous reservoir system, which allows complete cardiac flow support and blood oxygenation as well as hemodynamic stability during long-lasting procedures.
Methods: We present a retrospective case series of ten patients with valvular heart disease and unresponsive Ventricular Tachycardia (VT) who underwent VT ablation with MiECC support. The mean age of the patients was 72 ± 8 years and the left ventricular ejection fraction was 36 ± 12%. All patients underwent a clinical evaluation to identify the cause of VT unresponsiveness (e.g., ischemic heart disease).
Results: A total of 140 min, the following parameters were evaluated and recorded for 140 min. Central venous pressure (CVP) was used to evaluate excess volume. During the first 5 min, the mean was 15 mmHg, with a pump flow of 1.5 L/min and a mean systemic arterial pressure of 100 mmHg while setting up the circulation support. Following drainage in a volumetric bag of 1 L of blood, CVP was reduced to a value of 5 mmHg with a flow rate of 5 L/min and a mean systemic arterial pressure of 65 mmHg. In the case of small and low-weight patients our "1 L protocol" can be modified.
Conclusions: In this preliminary retrospective case series, the MiECC type III system may represent the ideal support system during VT ablation, and further studies are needed to support this preliminary report.
期刊介绍:
The Journal of Extracorporeal Technology is dedicated to the study and practice of Basic Science and Clinical issues related to extracorporeal circulation. Areas emphasized in the Journal include: •Cardiopulmonary Bypass •Cardiac Surgery •Cardiovascular Anesthesia •Hematology •Blood Management •Physiology •Fluid Dynamics •Laboratory Science •Coagulation and Hematology •Transfusion •Business Practices •Pediatric Perfusion •Total Quality Management • Evidence-Based Practices


 求助内容:
求助内容: 应助结果提醒方式:
应助结果提醒方式:


