Innovations in implementing a health systems response to violence against women in 3 tertiary hospitals of Maharashtra India: Improving provider capacity and facility readiness.
Srinivas Gadappa, Priya Prabhu, Sonali Deshpande, Nandkishor Gaikwad, Sanjida Arora, Sangeeta Rege, Sarah R Meyer, Claudia Garcia-Moreno, Avni Amin
{"title":"Innovations in implementing a health systems response to violence against women in 3 tertiary hospitals of Maharashtra India: Improving provider capacity and facility readiness.","authors":"Srinivas Gadappa, Priya Prabhu, Sonali Deshpande, Nandkishor Gaikwad, Sanjida Arora, Sangeeta Rege, Sarah R Meyer, Claudia Garcia-Moreno, Avni Amin","doi":"10.1177/26334895211067988","DOIUrl":null,"url":null,"abstract":"<p><strong>Background: </strong>Violence against women [VAW] is an urgent public health issue and health care providers [HCPs] are in a unique position to respond to such violence within a multi-sectoral health system response. In 2013, the World Health Organization (WHO) published clinical and policy guidelines (henceforth - the Guidelines) for responding to intimate partner violence and sexual violence against women. In this practical implementation report, we describe the adaptation of the Guidelines to train HCPs to respond to violence against women in tertiary health facilities in Maharashtra, India.</p><p><strong>Methods: </strong>We describe the strategies employed to adapt and implement the Guidelines, including participatory methods to identify and address HCPs' motivations and the barriers they face in providing care for women subjected to violence. The adaptation is built on querying health-systems level enablers and obstacles, as well as individual HCPs' perspectives on content and delivery of training and service delivery.</p><p><strong>Results: </strong>The training component of the intervention was delivered in a manner that included creating ownership among health managers who became champions for other health care providers; joint training across cadres to have clear roles, responsibilities and division of labour; and generating critical reflections about how gender power dynamics influence women's experience of violence and their health. The health systems strengthening activities included establishment of standard operating procedures [SOPs] for management of VAW and strengthening referrals to other services.</p><p><strong>Conclusions: </strong>In this intervention, standard training delivery was enhanced through participatory, joint and reflexive methods to generate critical reflection about gender, power and its influence on health outcomes. Training was combined with health system readiness activities to create an enabling environment. The lessons learned from this case study can be utilized to scale-up response in other levels of health facilities and states in India, as well as other LMIC contexts.</p><p><strong>Plain language summary: </strong>Violence against women affects millions of women globally. Health care providers may be able to support women in various ways, and finding ways to train and support health care providers in low and middle-income countries to provide high-quality care to women affected by violence is an urgent need. The WHO developed Clinical and Policy Guidelines in 2013, which provide guidance on how to improve health systems response to violence against women. We developed and implemented a series of interventions, including training of health care providers and innovations in service delivery, to implement the WHO guidelines for responding to violence against women in 3 tertiary hospitals of Maharashtra, India. The nascent published literature on health systems approaches to addressing violence against women in low and middle-income countries focuses on the impact of these interventions. This practical implementation report focuses on the interventions themselves, describes the processes of developing and adapting the intervention, and thus provides important insights for donors, policy-makers and researchers.</p>","PeriodicalId":73354,"journal":{"name":"Implementation research and practice","volume":"3 ","pages":"26334895211067988"},"PeriodicalIF":2.6000,"publicationDate":"2022-01-06","publicationTypes":"Journal Article","fieldsOfStudy":null,"isOpenAccess":false,"openAccessPdf":"https://ftp.ncbi.nlm.nih.gov/pub/pmc/oa_pdf/72/76/10.1177_26334895211067988.PMC9924251.pdf","citationCount":"0","resultStr":null,"platform":"Semanticscholar","paperid":null,"PeriodicalName":"Implementation research and practice","FirstCategoryId":"1085","ListUrlMain":"https://doi.org/10.1177/26334895211067988","RegionNum":0,"RegionCategory":null,"ArticlePicture":[],"TitleCN":null,"AbstractTextCN":null,"PMCID":null,"EPubDate":"2022/1/1 0:00:00","PubModel":"eCollection","JCR":"","JCRName":"","Score":null,"Total":0}
引用次数: 0
Abstract
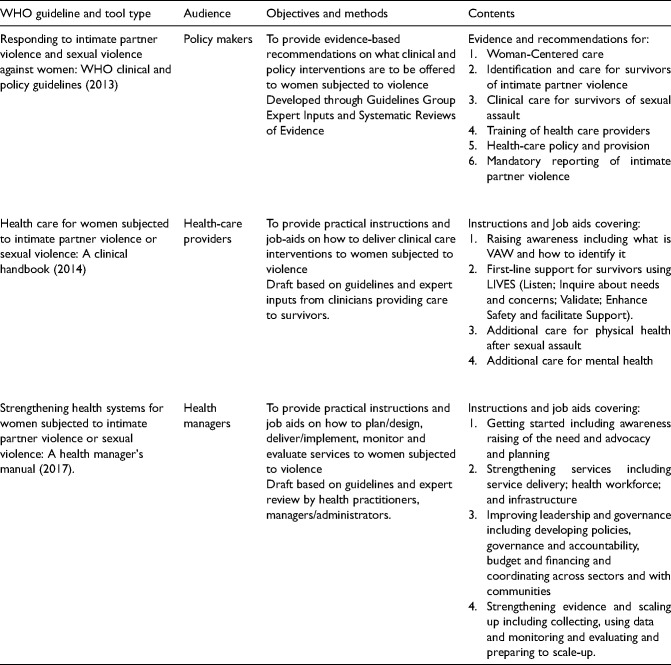
Background: Violence against women [VAW] is an urgent public health issue and health care providers [HCPs] are in a unique position to respond to such violence within a multi-sectoral health system response. In 2013, the World Health Organization (WHO) published clinical and policy guidelines (henceforth - the Guidelines) for responding to intimate partner violence and sexual violence against women. In this practical implementation report, we describe the adaptation of the Guidelines to train HCPs to respond to violence against women in tertiary health facilities in Maharashtra, India.
Methods: We describe the strategies employed to adapt and implement the Guidelines, including participatory methods to identify and address HCPs' motivations and the barriers they face in providing care for women subjected to violence. The adaptation is built on querying health-systems level enablers and obstacles, as well as individual HCPs' perspectives on content and delivery of training and service delivery.
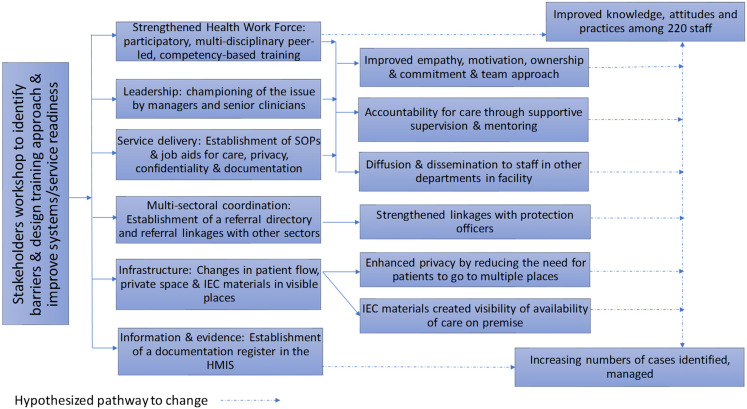
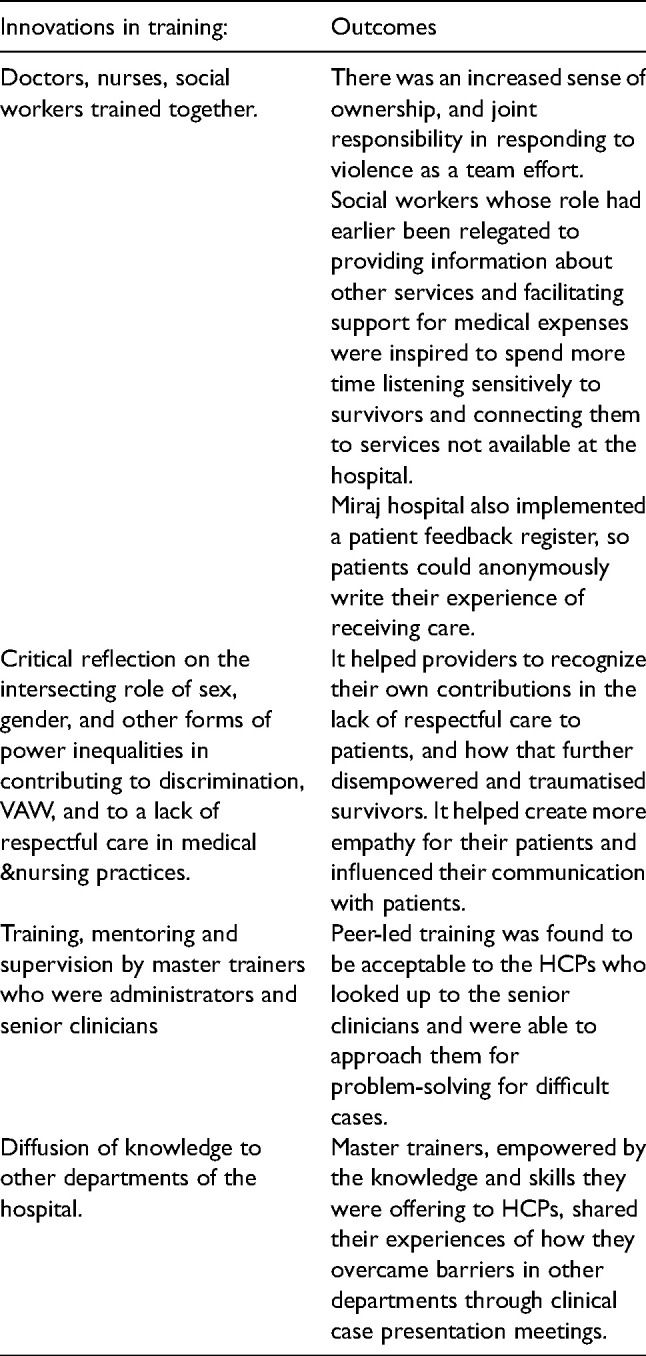
Results: The training component of the intervention was delivered in a manner that included creating ownership among health managers who became champions for other health care providers; joint training across cadres to have clear roles, responsibilities and division of labour; and generating critical reflections about how gender power dynamics influence women's experience of violence and their health. The health systems strengthening activities included establishment of standard operating procedures [SOPs] for management of VAW and strengthening referrals to other services.
Conclusions: In this intervention, standard training delivery was enhanced through participatory, joint and reflexive methods to generate critical reflection about gender, power and its influence on health outcomes. Training was combined with health system readiness activities to create an enabling environment. The lessons learned from this case study can be utilized to scale-up response in other levels of health facilities and states in India, as well as other LMIC contexts.
Plain language summary: Violence against women affects millions of women globally. Health care providers may be able to support women in various ways, and finding ways to train and support health care providers in low and middle-income countries to provide high-quality care to women affected by violence is an urgent need. The WHO developed Clinical and Policy Guidelines in 2013, which provide guidance on how to improve health systems response to violence against women. We developed and implemented a series of interventions, including training of health care providers and innovations in service delivery, to implement the WHO guidelines for responding to violence against women in 3 tertiary hospitals of Maharashtra, India. The nascent published literature on health systems approaches to addressing violence against women in low and middle-income countries focuses on the impact of these interventions. This practical implementation report focuses on the interventions themselves, describes the processes of developing and adapting the intervention, and thus provides important insights for donors, policy-makers and researchers.

 求助内容:
求助内容: 应助结果提醒方式:
应助结果提醒方式:


