Tanja Fens, Lisa de Jong, Bregt Kappelhoff, Cornelis Boersma, Maarten J Postma
{"title":"Budget and health impact of switching eligible patients with atrial fibrillation to lower- dose dabigatran.","authors":"Tanja Fens, Lisa de Jong, Bregt Kappelhoff, Cornelis Boersma, Maarten J Postma","doi":"10.1080/20016689.2023.2247719","DOIUrl":null,"url":null,"abstract":"<p><p><b>Objectives:</b> To assess the comparative budget and health impact of lower-dose dabigatran versus reduced doses of apixaban and rivaroxaban in atrial fibrillation (AF) patients eligible for a lower-/reduced-dose due to individual patient characteristics in the Netherlands. <b>Methods:</b> A budget impact model was developed in accordance with ISPOR guidelines. A 3-year-time horizon was considered, and analyses were conducted from a Dutch healthcare payer's perspective. The model applies published data to local AF-epidemiology, allowing calculations to estimate clinical events (strokes and haemorrhages) and costs. The analyses were based on real-world outcomes from patients with AF receiving a first direct oral anticoagulant (DOAC) prescription for low-dose dabigatran (110 mg) and a reduced dose of apixaban (2.5 mg) or rivaroxaban (15 mg). Two situations of switching treatments from one to another DOAC were modelled: switching from apixaban to dabigatran and from rivaroxaban to dabigatran. Base case results were given as savings per 100 patient-year, per total Dutch population, and events avoided. A univariate sensitivity analysis was conducted to explore the uncertainty around epidemiological and event costs input data. Scenario analyses were performed to estimate the effect of different market shares and potential price reductions due to future patent expiry for the total real-world population from the Netherlands. <b>Results:</b> The 3-years outcomes of switching patients eligible for a lower-/reduced-dose due to individual patient characteristics from apixaban or rivaroxaban to dabigatran resulted in cost savings estimated at €157 or €72 thousand per 100 patient-years, respectively, or €146 million per total Dutch population. Looking into the clinical events, dabigatran reflected the lowest number of mortalities, ischemic strokes, major bleeding, non-major bleeding, and haemorrhagic stroke compared to apixaban and rivaroxaban. The sensitivity analysis consistently reflected cost savings, with the ischeamic stroke events having the biggest impact. Accounting for the Dutch situation, both scenarios showed total savings ranging from €45 to €229 million over 3 years. <b>Conclusions:</b> Switching eligible AF-patients from reduced-dose apixaban or rivaroxaban to lower-dose dabigatran has the potential to reduce healthcare payer's budget expenditures and provide health gains. Cost savings can potentially be further enhanced by market share adjustments and further price reductions.</p>","PeriodicalId":73811,"journal":{"name":"Journal of market access & health policy","volume":"11 1","pages":"2247719"},"PeriodicalIF":0.0000,"publicationDate":"2023-01-01","publicationTypes":"Journal Article","fieldsOfStudy":null,"isOpenAccess":false,"openAccessPdf":"https://ftp.ncbi.nlm.nih.gov/pub/pmc/oa_pdf/e1/da/ZJMA_11_2247719.PMC10478629.pdf","citationCount":"0","resultStr":null,"platform":"Semanticscholar","paperid":null,"PeriodicalName":"Journal of market access & health policy","FirstCategoryId":"1085","ListUrlMain":"https://doi.org/10.1080/20016689.2023.2247719","RegionNum":0,"RegionCategory":null,"ArticlePicture":[],"TitleCN":null,"AbstractTextCN":null,"PMCID":null,"EPubDate":"","PubModel":"","JCR":"Q2","JCRName":"Medicine","Score":null,"Total":0}
引用次数: 0
Abstract
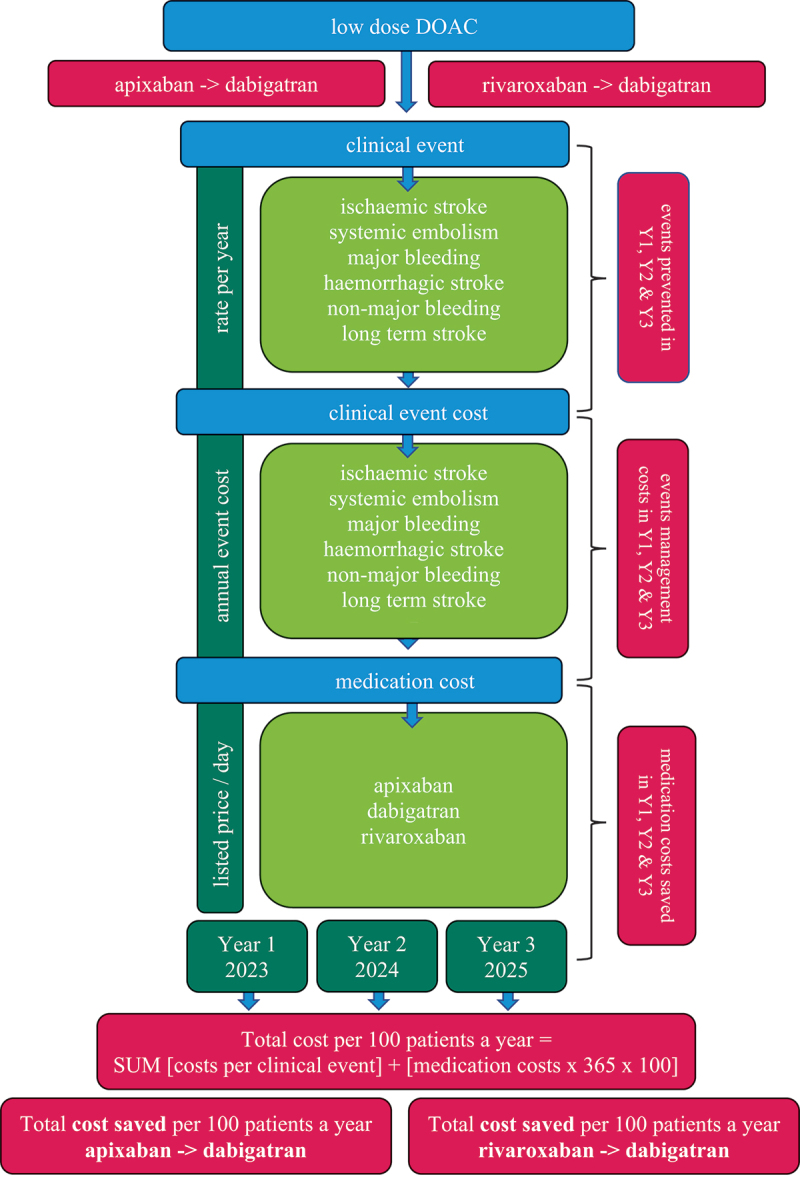
Objectives: To assess the comparative budget and health impact of lower-dose dabigatran versus reduced doses of apixaban and rivaroxaban in atrial fibrillation (AF) patients eligible for a lower-/reduced-dose due to individual patient characteristics in the Netherlands. Methods: A budget impact model was developed in accordance with ISPOR guidelines. A 3-year-time horizon was considered, and analyses were conducted from a Dutch healthcare payer's perspective. The model applies published data to local AF-epidemiology, allowing calculations to estimate clinical events (strokes and haemorrhages) and costs. The analyses were based on real-world outcomes from patients with AF receiving a first direct oral anticoagulant (DOAC) prescription for low-dose dabigatran (110 mg) and a reduced dose of apixaban (2.5 mg) or rivaroxaban (15 mg). Two situations of switching treatments from one to another DOAC were modelled: switching from apixaban to dabigatran and from rivaroxaban to dabigatran. Base case results were given as savings per 100 patient-year, per total Dutch population, and events avoided. A univariate sensitivity analysis was conducted to explore the uncertainty around epidemiological and event costs input data. Scenario analyses were performed to estimate the effect of different market shares and potential price reductions due to future patent expiry for the total real-world population from the Netherlands. Results: The 3-years outcomes of switching patients eligible for a lower-/reduced-dose due to individual patient characteristics from apixaban or rivaroxaban to dabigatran resulted in cost savings estimated at €157 or €72 thousand per 100 patient-years, respectively, or €146 million per total Dutch population. Looking into the clinical events, dabigatran reflected the lowest number of mortalities, ischemic strokes, major bleeding, non-major bleeding, and haemorrhagic stroke compared to apixaban and rivaroxaban. The sensitivity analysis consistently reflected cost savings, with the ischeamic stroke events having the biggest impact. Accounting for the Dutch situation, both scenarios showed total savings ranging from €45 to €229 million over 3 years. Conclusions: Switching eligible AF-patients from reduced-dose apixaban or rivaroxaban to lower-dose dabigatran has the potential to reduce healthcare payer's budget expenditures and provide health gains. Cost savings can potentially be further enhanced by market share adjustments and further price reductions.

 求助内容:
求助内容: 应助结果提醒方式:
应助结果提醒方式:


