Melanoma patients with immune-related adverse events after immune checkpoint inhibitors are characterized by a distinct immunological phenotype of circulating T cells and M-MDSCs.
{"title":"Melanoma patients with immune-related adverse events after immune checkpoint inhibitors are characterized by a distinct immunological phenotype of circulating T cells and M-MDSCs.","authors":"Alisa Lepper, Rebekka Bitsch, Feyza Gül Özbay Kurt, Ihor Arkhypov, Samantha Lasser, Jochen Utikal, Viktor Umansky","doi":"10.1080/2162402X.2023.2247303","DOIUrl":null,"url":null,"abstract":"<p><p>Treatment with immune checkpoint inhibitors (ICIs) has improved the prognosis of melanoma patients. However, ICIs can cause an overactivation of the immune system followed by diverse immunological side effects known as immune-related adverse events (irAE). Currently, the toxicity of irAE is limiting the usage of ICIs. Here, we studied circulating monocytic myeloid-derived suppressor cells (M-MDSCs) and T cells in course of irAE after the ICI therapy. Our longitudinal study involved 31 melanoma patients with and without adverse events during anti-PD-1 monotherapy or anti-CTLA-4/PD-1 combination therapy. Peripheral blood samples were analyzed before ICI start, during ICI treatment, at the time point of irAE and during immunosuppressive treatment to cure irAE. We observed an enhanced progression-free survival among patients with irAE. In patients with irAE, we found an upregulation of CD69 on CD8<sup>+</sup> T cells and a decreased frequency of regulatory T cells (Tregs). Moreover, lower frequencies of Tregs correlated with more severe side effects. Patients treated with immunomodulatory drugs after irAE manifestation tend to show an elevated number of M-MDSCs during an immunosuppressive therapy. We suggest that an activation of CD8<sup>+</sup> T cells and the reduction of Treg frequencies could be responsible for the development of irAE.</p>","PeriodicalId":19683,"journal":{"name":"Oncoimmunology","volume":"12 1","pages":"2247303"},"PeriodicalIF":7.2000,"publicationDate":"2023-08-13","publicationTypes":"Journal Article","fieldsOfStudy":null,"isOpenAccess":false,"openAccessPdf":"https://ftp.ncbi.nlm.nih.gov/pub/pmc/oa_pdf/6b/05/KONI_12_2247303.PMC10431726.pdf","citationCount":"0","resultStr":null,"platform":"Semanticscholar","paperid":null,"PeriodicalName":"Oncoimmunology","FirstCategoryId":"3","ListUrlMain":"https://doi.org/10.1080/2162402X.2023.2247303","RegionNum":2,"RegionCategory":"医学","ArticlePicture":[],"TitleCN":null,"AbstractTextCN":null,"PMCID":null,"EPubDate":"2023/1/1 0:00:00","PubModel":"eCollection","JCR":"","JCRName":"","Score":null,"Total":0}
引用次数: 0
Abstract
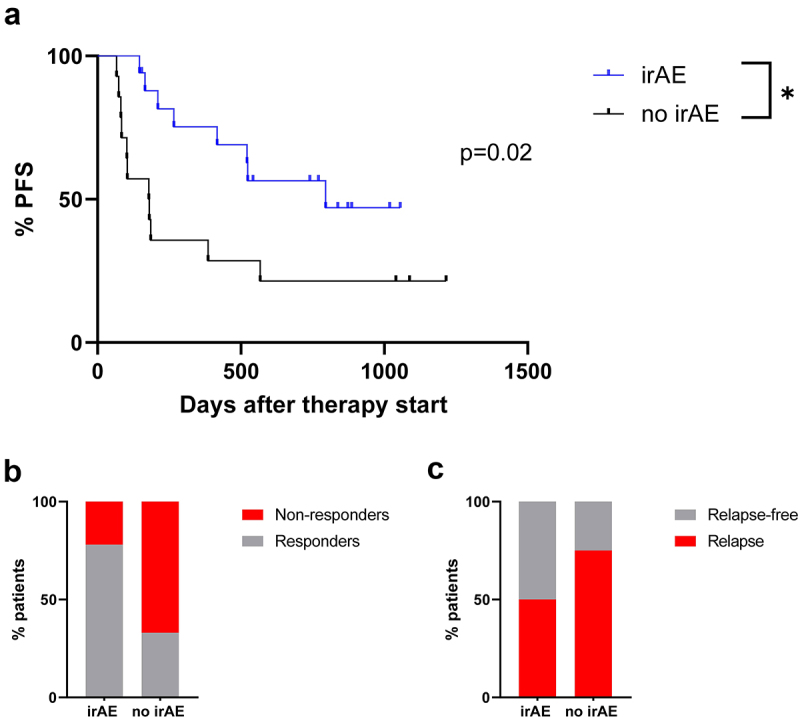
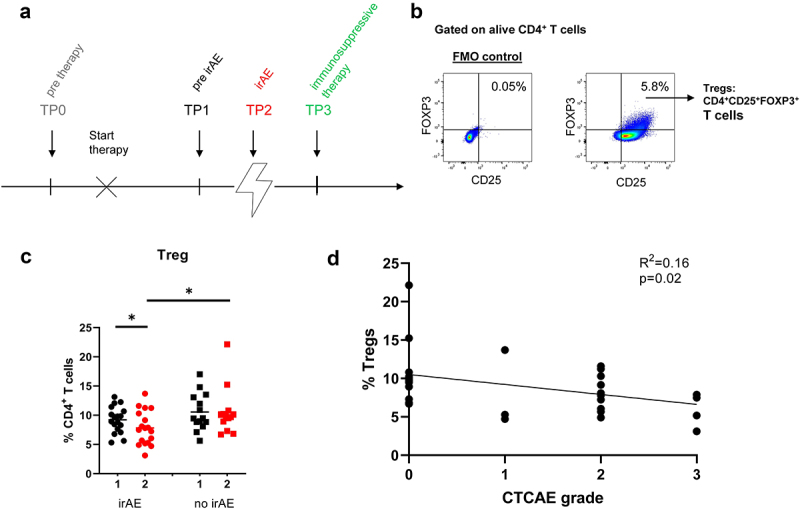
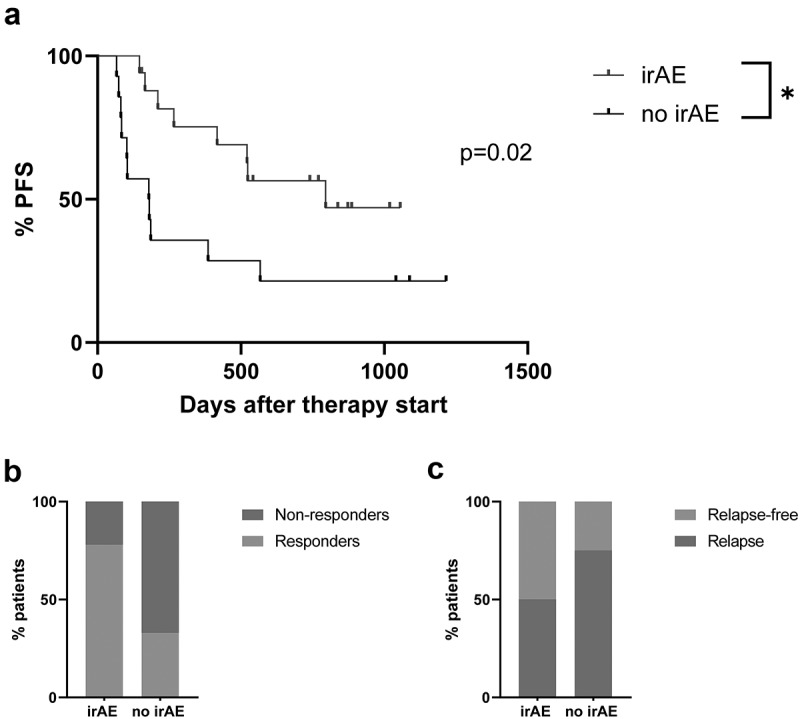
Treatment with immune checkpoint inhibitors (ICIs) has improved the prognosis of melanoma patients. However, ICIs can cause an overactivation of the immune system followed by diverse immunological side effects known as immune-related adverse events (irAE). Currently, the toxicity of irAE is limiting the usage of ICIs. Here, we studied circulating monocytic myeloid-derived suppressor cells (M-MDSCs) and T cells in course of irAE after the ICI therapy. Our longitudinal study involved 31 melanoma patients with and without adverse events during anti-PD-1 monotherapy or anti-CTLA-4/PD-1 combination therapy. Peripheral blood samples were analyzed before ICI start, during ICI treatment, at the time point of irAE and during immunosuppressive treatment to cure irAE. We observed an enhanced progression-free survival among patients with irAE. In patients with irAE, we found an upregulation of CD69 on CD8+ T cells and a decreased frequency of regulatory T cells (Tregs). Moreover, lower frequencies of Tregs correlated with more severe side effects. Patients treated with immunomodulatory drugs after irAE manifestation tend to show an elevated number of M-MDSCs during an immunosuppressive therapy. We suggest that an activation of CD8+ T cells and the reduction of Treg frequencies could be responsible for the development of irAE.
期刊介绍:
Tumor immunology explores the natural and therapy-induced recognition of cancers, along with the complex interplay between oncogenesis, inflammation, and immunosurveillance. In response to recent advancements, a new journal, OncoImmunology, is being launched to specifically address tumor immunology. The field has seen significant progress with the clinical demonstration and FDA approval of anticancer immunotherapies. There's also growing evidence suggesting that many current chemotherapeutic agents rely on immune effectors for their efficacy.
While oncologists have historically utilized chemotherapeutic and radiotherapeutic regimens successfully, they may have unwittingly leveraged the immune system's ability to recognize tumor-specific antigens and control cancer growth. Consequently, immunological biomarkers are increasingly crucial for cancer prognosis and predicting chemotherapy efficacy. There's strong support for combining conventional anticancer therapies with immunotherapies. OncoImmunology will welcome high-profile submissions spanning fundamental, translational, and clinical aspects of tumor immunology, including solid and hematological cancers, inflammation, and both innate and acquired immune responses.
 求助内容:
求助内容: 应助结果提醒方式:
应助结果提醒方式:


