{"title":"Changes in receipt of adjuvant brachytherapy for endometrial cancer patients before and after affordable care act: The impact of Medicaid expansion.","authors":"Amy Le, Jordan A Holmes","doi":"10.5114/jcb.2023.127838","DOIUrl":null,"url":null,"abstract":"<p><strong>Purpose: </strong>For patients with high-intermediate risk (HIR) endometrial cancer, adjuvant radiation (RT) reduces the risk of recurrence, but many patients do not receive RT. Under the Affordable Care Act (ACA), most states expanded Medicaid coverage. Our hypothesis was patients would be more likely to receive indicated adjuvant RT in states that expanded Medicaid compared with patients in states that did not expand Medicaid.</p><p><strong>Material and methods: </strong>National Cancer Database (NCDB) was used to identify patients aged 40-64 years with HIR endometrial adenocarcinoma, stage IA and grade 3 or stage IB and grade 1 or 2, diagnosed from 2010-2018. We conducted a difference-in-differences (DID) cross-sectional retrospective analysis comparing receipt of adjuvant RT among patients residing in Medicaid expansion and non-expansion states before and after ACA implementation (January 2014).</p><p><strong>Results: </strong>Expansion states had higher rates of adjuvant RT prior to January 2014 compared with non-expansion states (49.21% vs. 36.46%), and the proportion of patients who received adjuvant RT increased over the study period across both Medicaid expansion and non-expansion states. After Medicaid expansion, the non-expansion states had a larger absolute increase in adjuvant radiation resulting in a non-significant change in the difference in adjuvant radiation rates compared with baseline (crude increase: 9.63% vs. 7.45%, adjusted DID: -2.68 [95% CI: -7.12-1.75], <i>p</i> = 0.236).</p><p><strong>Conclusions: </strong>Medicaid expansion is likely not the most significant factor affecting access or receipt of adjuvant RT for HIR endometrial cancer patients. Further study could help inform policy and efforts to ensure all patients have access to guideline-recommended RT.</p>","PeriodicalId":51305,"journal":{"name":"Journal of Contemporary Brachytherapy","volume":"15 3","pages":"206-211"},"PeriodicalIF":1.1000,"publicationDate":"2023-06-01","publicationTypes":"Journal Article","fieldsOfStudy":null,"isOpenAccess":false,"openAccessPdf":"https://ftp.ncbi.nlm.nih.gov/pub/pmc/oa_pdf/8d/ae/JCB-15-50785.PMC10324593.pdf","citationCount":"0","resultStr":null,"platform":"Semanticscholar","paperid":null,"PeriodicalName":"Journal of Contemporary Brachytherapy","FirstCategoryId":"3","ListUrlMain":"https://doi.org/10.5114/jcb.2023.127838","RegionNum":4,"RegionCategory":"医学","ArticlePicture":[],"TitleCN":null,"AbstractTextCN":null,"PMCID":null,"EPubDate":"","PubModel":"","JCR":"Q4","JCRName":"ONCOLOGY","Score":null,"Total":0}
引用次数: 0
Abstract
Purpose: For patients with high-intermediate risk (HIR) endometrial cancer, adjuvant radiation (RT) reduces the risk of recurrence, but many patients do not receive RT. Under the Affordable Care Act (ACA), most states expanded Medicaid coverage. Our hypothesis was patients would be more likely to receive indicated adjuvant RT in states that expanded Medicaid compared with patients in states that did not expand Medicaid.
Material and methods: National Cancer Database (NCDB) was used to identify patients aged 40-64 years with HIR endometrial adenocarcinoma, stage IA and grade 3 or stage IB and grade 1 or 2, diagnosed from 2010-2018. We conducted a difference-in-differences (DID) cross-sectional retrospective analysis comparing receipt of adjuvant RT among patients residing in Medicaid expansion and non-expansion states before and after ACA implementation (January 2014).
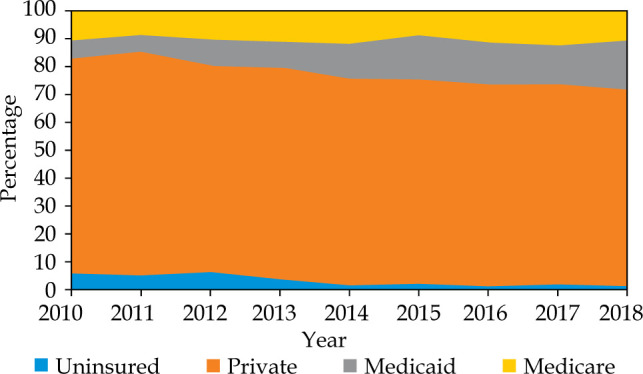
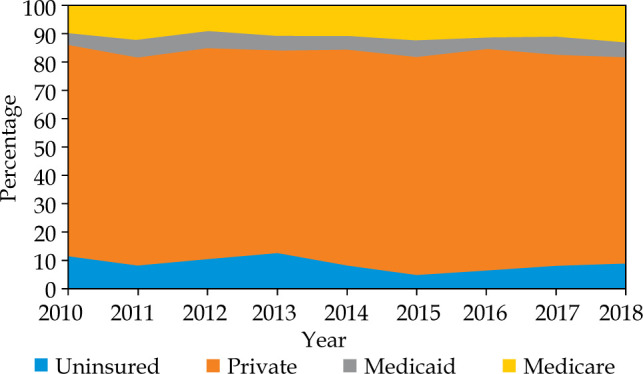
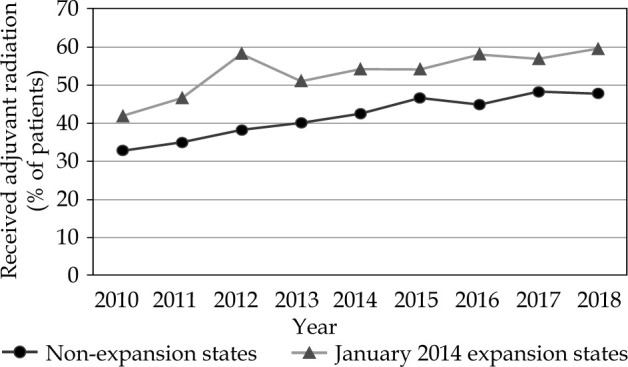
Results: Expansion states had higher rates of adjuvant RT prior to January 2014 compared with non-expansion states (49.21% vs. 36.46%), and the proportion of patients who received adjuvant RT increased over the study period across both Medicaid expansion and non-expansion states. After Medicaid expansion, the non-expansion states had a larger absolute increase in adjuvant radiation resulting in a non-significant change in the difference in adjuvant radiation rates compared with baseline (crude increase: 9.63% vs. 7.45%, adjusted DID: -2.68 [95% CI: -7.12-1.75], p = 0.236).
Conclusions: Medicaid expansion is likely not the most significant factor affecting access or receipt of adjuvant RT for HIR endometrial cancer patients. Further study could help inform policy and efforts to ensure all patients have access to guideline-recommended RT.
目的:对于中高风险(HIR)子宫内膜癌患者,辅助放疗(RT)可降低复发风险,但许多患者不接受RT。根据平价医疗法案(ACA),大多数州扩大了医疗补助覆盖范围。我们的假设是,与没有扩大医疗补助的州相比,扩大医疗补助的州的患者更有可能接受指示性辅助放疗。材料和方法:使用国家癌症数据库(NCDB)识别2010-2018年诊断的40-64岁HIR子宫内膜腺癌患者,IA期和3级或IB期和1或2级。我们进行了差异中的差异(DID)横断面回顾性分析,比较了ACA实施前后(2014年1月)居住在医疗补助扩张州和非扩张州的患者接受辅助RT的情况。结果:2014年1月之前,扩展州的辅助放疗率高于非扩展州(49.21%对36.46%),并且在研究期间,医疗补助扩展州和非扩展州接受辅助放疗的患者比例都有所增加。在医疗补助扩大后,未扩大的州有更大的辅助放疗绝对增加,导致辅助放疗率与基线相比差异无显著变化(粗增加:9.63% vs. 7.45%,调整后的DID: -2.68 [95% CI: -7.12-1.75], p = 0.236)。结论:医疗补助扩大可能不是影响HIR子宫内膜癌患者获得或接受辅助放疗的最重要因素。进一步的研究可以为政策和努力提供信息,确保所有患者都能获得指南推荐的RT。
期刊介绍:
The “Journal of Contemporary Brachytherapy” is an international and multidisciplinary journal that will publish papers of original research as well as reviews of articles. Main subjects of the journal include: clinical brachytherapy, combined modality treatment, advances in radiobiology, hyperthermia and tumour biology, as well as physical aspects relevant to brachytherapy, particularly in the field of imaging, dosimetry and radiation therapy planning. Original contributions will include experimental studies of combined modality treatment, tumor sensitization and normal tissue protection, molecular radiation biology, and clinical investigations of cancer treatment in brachytherapy. Another field of interest will be the educational part of the journal.

 求助内容:
求助内容: 应助结果提醒方式:
应助结果提醒方式:


