Abbey Studer, Barbara Fleming, Roderick C Jones, Audrey Rosenblatt, Lisa Sohn, Megan Ivey, Marleta Reynolds, Gustave H Falciglia
{"title":"Reducing Intraoperative Hypothermia in Infants from the Neonatal Intensive Care Unit.","authors":"Abbey Studer, Barbara Fleming, Roderick C Jones, Audrey Rosenblatt, Lisa Sohn, Megan Ivey, Marleta Reynolds, Gustave H Falciglia","doi":"10.1097/pq9.0000000000000665","DOIUrl":null,"url":null,"abstract":"<p><p>Infants from the neonatal intensive care unit (NICU) undergoing surgery in the operating room (OR) are at greater risk for hypothermia during surgery than afterward due to environmental heat loss, anesthesia, and inconsistent temperature monitoring. A multidisciplinary team aimed to reduce hypothermia (<36.1 °C) for infants at a level IV NICU at the beginning of the operation (first OR temperature) or at any time during the operation (lowest OR temperature) by 25%.</p><p><strong>Methods: </strong>The team followed preoperative, intraoperative (first, lowest, and last OR), and postoperative temperatures. It sought to reduce intraoperative hypothermia using the \"Model for Improvement\" by standardizing temperature monitoring, transport, and OR warming, including raising ambient OR temperatures to 74°F. Temperature monitoring was continuous, secure, and automated. The balancing metric was postoperative hyperthermia (>38 °C).</p><p><strong>Results: </strong>Over 4 years, there were 1235 operations: 455 in the baseline and 780 in the intervention period. The percentage of infants experiencing hypothermia upon OR arrival and at any point during the operation decreased from 48.7% to 6.4% and 67.5% to 37.4%, respectively. Upon return to the NICU, the percentage of infants experiencing postoperative hypothermia decreased from 5.8% to 2.1%, while postoperative hyperthermia increased from 0.8% to 2.6%.</p><p><strong>Conclusions: </strong>Intraoperative hypothermia is more prevalent than postoperative hypothermia. Standardizing temperature monitoring, transport, and OR warming reduces both; however, further reduction requires a better understanding of how and when risk factors contribute to hypothermia to avoid further increasing hyperthermia. Continuous, secure, and automated data collection improved temperature management by enhancing situational awareness and facilitating data analysis.</p>","PeriodicalId":74412,"journal":{"name":"Pediatric quality & safety","volume":null,"pages":null},"PeriodicalIF":1.2000,"publicationDate":"2023-07-01","publicationTypes":"Journal Article","fieldsOfStudy":null,"isOpenAccess":false,"openAccessPdf":"https://ftp.ncbi.nlm.nih.gov/pub/pmc/oa_pdf/d6/48/pqs-8-e655.PMC10332830.pdf","citationCount":"0","resultStr":null,"platform":"Semanticscholar","paperid":null,"PeriodicalName":"Pediatric quality & safety","FirstCategoryId":"1085","ListUrlMain":"https://doi.org/10.1097/pq9.0000000000000665","RegionNum":0,"RegionCategory":null,"ArticlePicture":[],"TitleCN":null,"AbstractTextCN":null,"PMCID":null,"EPubDate":"","PubModel":"","JCR":"Q3","JCRName":"PEDIATRICS","Score":null,"Total":0}
引用次数: 0
Abstract
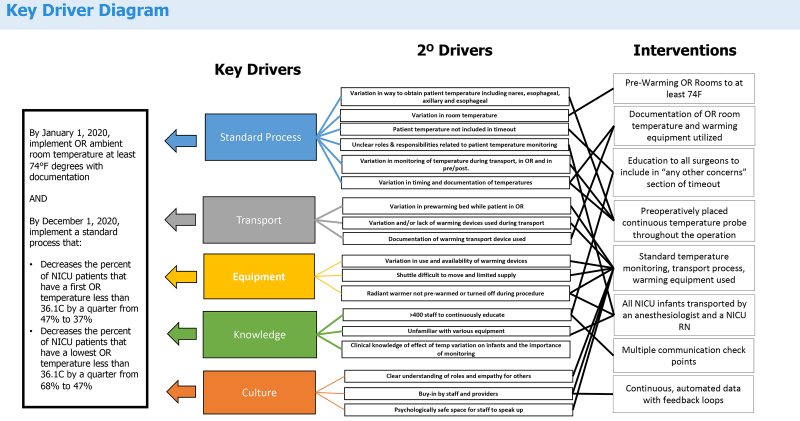
Infants from the neonatal intensive care unit (NICU) undergoing surgery in the operating room (OR) are at greater risk for hypothermia during surgery than afterward due to environmental heat loss, anesthesia, and inconsistent temperature monitoring. A multidisciplinary team aimed to reduce hypothermia (<36.1 °C) for infants at a level IV NICU at the beginning of the operation (first OR temperature) or at any time during the operation (lowest OR temperature) by 25%.
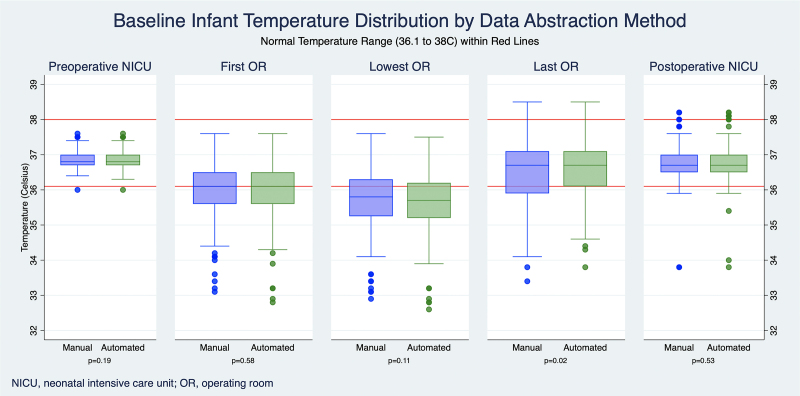
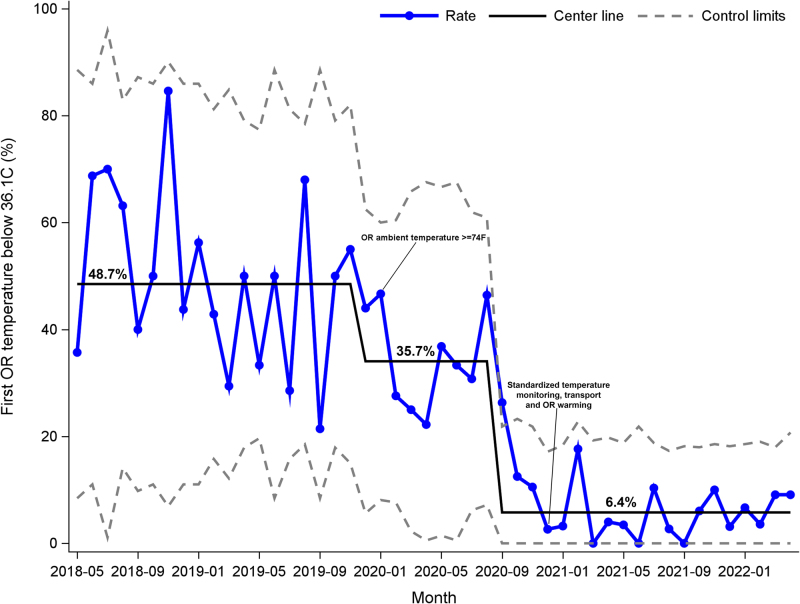
Methods: The team followed preoperative, intraoperative (first, lowest, and last OR), and postoperative temperatures. It sought to reduce intraoperative hypothermia using the "Model for Improvement" by standardizing temperature monitoring, transport, and OR warming, including raising ambient OR temperatures to 74°F. Temperature monitoring was continuous, secure, and automated. The balancing metric was postoperative hyperthermia (>38 °C).
Results: Over 4 years, there were 1235 operations: 455 in the baseline and 780 in the intervention period. The percentage of infants experiencing hypothermia upon OR arrival and at any point during the operation decreased from 48.7% to 6.4% and 67.5% to 37.4%, respectively. Upon return to the NICU, the percentage of infants experiencing postoperative hypothermia decreased from 5.8% to 2.1%, while postoperative hyperthermia increased from 0.8% to 2.6%.
Conclusions: Intraoperative hypothermia is more prevalent than postoperative hypothermia. Standardizing temperature monitoring, transport, and OR warming reduces both; however, further reduction requires a better understanding of how and when risk factors contribute to hypothermia to avoid further increasing hyperthermia. Continuous, secure, and automated data collection improved temperature management by enhancing situational awareness and facilitating data analysis.

 求助内容:
求助内容: 应助结果提醒方式:
应助结果提醒方式:


